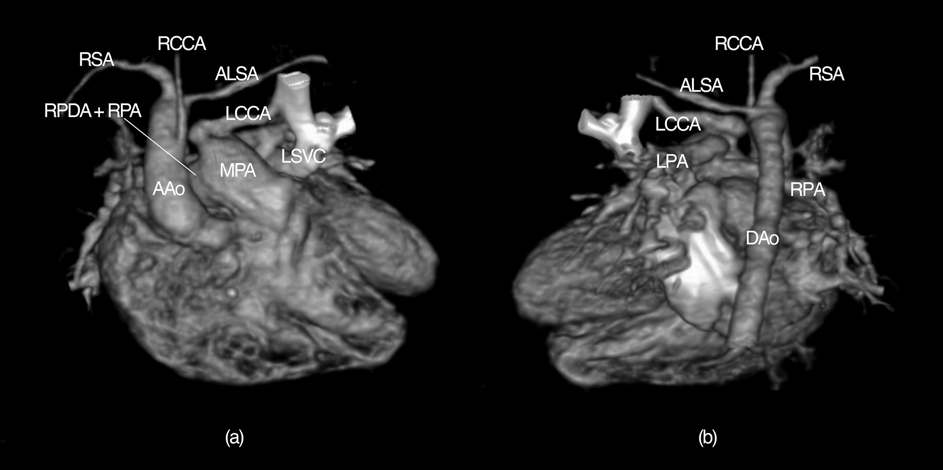
The patient, born at 35 weeks’ gestation with a double outlet right ventricle, ventricular septal defect and persistent left superior vena cava, was referred to our institution. The baby showed critical airway obstruction immediately after birth due to pharyngeal and laryngeal hypoplasia, and necessitated emergent tracheostomy, as well as a surgical correction for the esophageal atresia prior to the reference. On physical examination, the heart rate was regular at 142 beats/min, and pulse oximetry showed oxygen saturation of 95% in room air. A grade 3/6 systolic murmur was best noted at the left midsternal border. Several peculiar clinical observations, including agenesis of the thymus and hypocalcemia associated with cleft palate and a dysmorphic face, indicated that she had chromosome 22q11.2 deletion syndrome. A chest X-ray film showed increased pulmonary vascular shadow. Enhanced multi-slice helical CT and three-dimensional image reconstruction revealed the presence of a right aortic arch with an anomalous left subclavian artery originating from the descending aorta. She had a left superior vena cava with absence of an innominate vein. A right patent ductus arteriosus was also seen. The first branch from the aortic arch, running toward the right cervix, was concluded to be the right common carotid artery. An anomalous artery, connecting to the antero-cranial aspect of the pulmonary artery bifurcation, and leading to the left cervix, was deduced to be the left common carotid artery (Fig. 1).
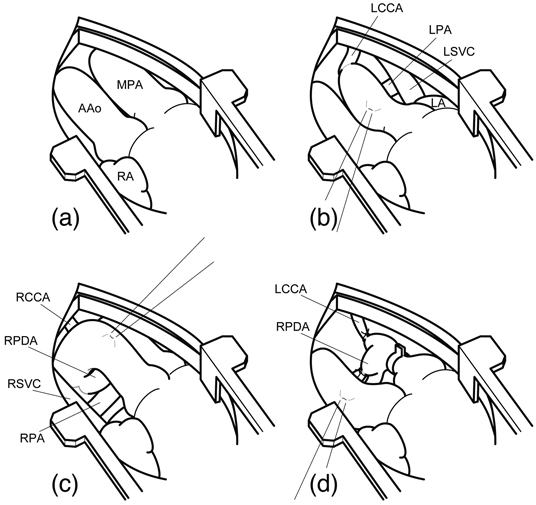
The baby underwent an operation via a lower partial sternotomy at 19 days of age. We found the gross anatomy consisted of a double outlet right ventricle, locating the aorta and the pulmonary artery side by side. Ligation of the right patent ductus arteriosus and pulmonary artery banding were performed, followed by a simple ligation of the left common carotid artery (Fig. 2). A near-infrared spectroscopy (INVOS 5100C, Covidien Inc., USA) showed no abnormal changes in the cerebral oxygenation status during the procedures. The post-operative course was uneventful.
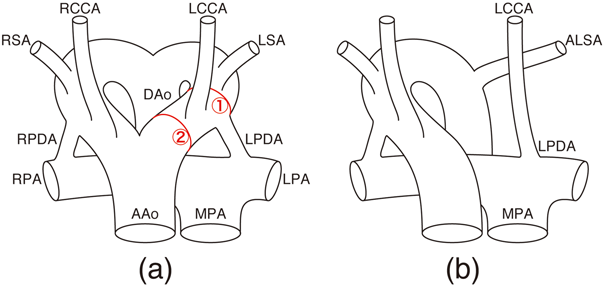
Since the first case of an isolated left common carotid artery was reported in 1987, six cases have been described in the literature.1–3) Each case has a right aortic arch and an aberrant left subclavian artery with the isolated left common carotid artery connecting to the pulmonary artery. As well as significant congenital cardiac defects, chromosome deletion syndromes were highly associated in most cases, including chromosome 22q11.2 deletion, or DiGeorge syndrome. The etiologic basis for this association is thought to be a failure of derivatives of the cephalic neural crest, followed by a failure in the aorticopulmonary septation and thymic morphogenesis during early embryogenesis.4) The Edwards’ double aortic arch model well explains anomalies in aortic arch branching by selective regression of various parts of vessels.5) In our case, while a break occurred between the left subclavian and the left carotid arteries, resulting in a right aortic arch with an aberrant left subclavian artery, a second break appeared between the aortic sac and the left carotid artery. This combination of regression produces an isolated left common carotid artery and would allow this third arch derivative to join the pulmonary artery, mediating the left patent ductus arteriosus1, 5) (Fig. 3).
In the operation, we made a simple ligation of the isolated common carotid artery to abolish the pulmonary steal phenomenon to which the cerebral circulation is subjected by this vascular arrangement. Re-implantation of the artery to the aorta or either of the arch branches was dismissed because a preceding tracheostomy prevented full exposure and mobilization of the vessels.
We report the very rare case of aortic arch anomalies, that is isolated left common carotid artery from the main pulmonary artery. To the best of our knowledge, this is the seventh case in the English-language literature.
 1,Satoru Kawai2,Noritaka Okada1,Hideyuki Okawa1,Kazushi Yasuda2Hiroomi Murayama
1,Satoru Kawai2,Noritaka Okada1,Hideyuki Okawa1,Kazushi Yasuda2Hiroomi Murayama