The Ross procedure is a satisfactory surgical treatment for young patients who need aortic valve replacement. On the other hand, autograft dysfunction and autograft aneurysm were observed in 30–40% of late survivors, and 10% of patients required autograft reoperation.1, 2) Several modified techniques are proposed including root fixation to prevent root dilation;3) however, a supported root technique may not be sufficient to avoid sinus of Valsalva dilation. For valve-sparing root replacement operation, David technique is commonly favored to stabilize the dilated autograft annulus and to replace the aortic root.
Here we present a case of distal autograft aneurysm successfully treated with valve-sparing root replacement with Yacoub technique, 20 years after the Ross procedure with root fixation.
A 45-year-old male scheduled for thyroid tumor resection was referred to our institution for ascending aortic aneurysm, distal autograft aneurysm and right ventricle to pulmonary artery (RV-PA) conduit stenosis. He underwent the Ross procedure with aortic root fixation by Dacron felt 20 years previously for valvular aortic stenosis and regurgitation related with bicuspid aortic valve. No reinforcement material was utilized for the distal suture line, and the right ventricular outflow tract was reconstructed with a 30-mm bicuspid pericardial roll conduit. His postoperative recovery after the Ross procedure was uneventful; however, he was lost for follow-up after a few routine clinic visits. His autograft aneurysm was revealed coincidentally by preoperative chest CT scan for thyroid tumor.
His past medical history is significant for hypertension, treated with azilsartan and amlodipine. Blood test was normal except elevated BNP of 32.5 pg/mL. An electrocardiogram showed first-degree atrioventricular block and incomplete right bundle branch block. His chest X-ray revealed wide mediastinum.
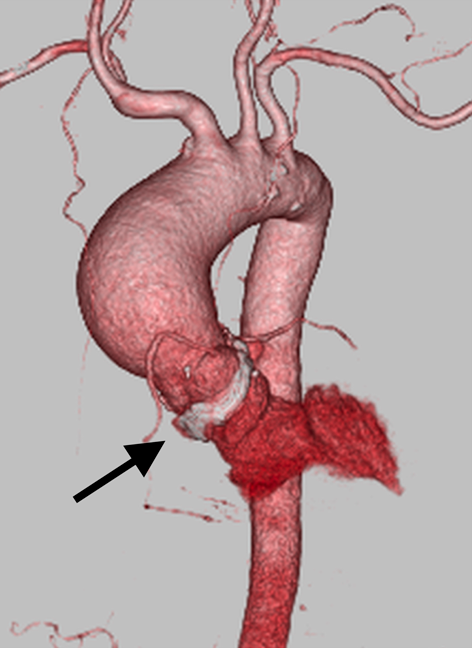
A transthoracic echocardiogram showed ascending aortic aneurysm of 53 mm, autograft aneurysm with sinus of Valsalva diameter of 45 mm, normal (27 mm) aortic annulus, mild autograft regurgitation, globally reduced left ventricular function with ejection fraction of 49%, mild RV-PA conduit stenosis (peak pressure gradient of 22 mmHg) and normal right ventricular function. A computed tomography (CT) scan revealed ascending aortic aneurysm of 58 mm with distal sinus of Valsalva diameter of 47 mm. His aortic root was fixed with mildly calcified Dacron felt (Fig. 1).
In the setting of significant aneurysm of the autograft and ascending aorta and mild RV-PA conduit stenosis, valve-sparing aortic root replacement by David technique and RV-PA conduit replacement were planned.
Reoperation was performed through a redo median sternotomy and under normothermic cardiopulmonary bypass with bicaval cannulation. After aortic cross-clamp and cardiac arrest, the RV-PA conduit was excised, and the ascending aorta was transected. The dilatation began just distal to the commissures of the aortic valve, and the previous distal suture line of autograft was identified in the aneurysmal portion. Since this patient had distal autograft aneurysmal dilatation, the autograft wall still carried the risk of future aneurysm formation. Therefore, we decided to remove as much autograft tissue as possible. The aneurysm wall was excised and the coronary buttons were harvested by incising the suture lines at the Ross procedure. However, the aortic root and Dacron felt were severely calcified, and it was impossible to dissect the aortic root or to put the needle through the Dacron felt.
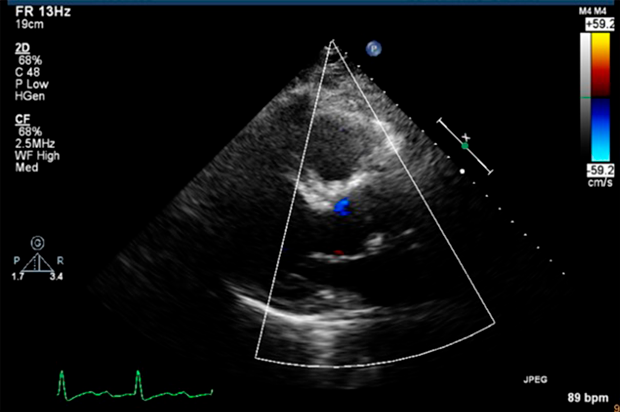
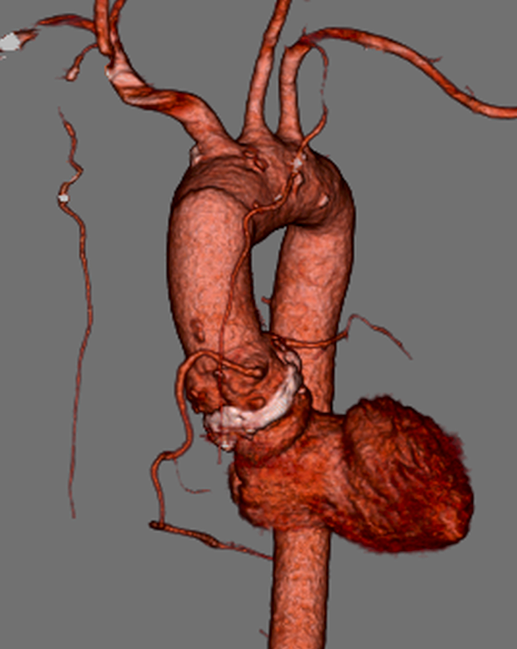
Since David technique seemed very challenging and the aortic root seemed well stabilized with previous fixation material, the plan was changed to proceed with Yacoub technique. Size of Dacron Valsalva graft was chosen based on the normal portion of sinus of Valsalva just below the commissure of the aortic valve. A 30-mm Dacron Valsalva graft was fashioned into scalloped shape and anastomosed to the autograft with 4–0 polypropylene continuous suture in end-to-end fashion. The coronary buttons were anastomosed to the side-holes created on the Valsalva graft, and the graft was anastomosed to distal ascending aorta. The RV-PA conduit was replaced with 24-mm tricuspid expanded polytetrafluoroethylene conduit with bulging sinuses. The weaning from cardiopulmonary bypass and his postoperative course were uneventful. He was discharged to home on the 19th postoperative day. His follow up transthoracic echocardiogram and chest CT scan revealed nicely reconstructed aorta, trivial to mild aortic valve regurgitation and well reconstructed RV-PA conduit (Figs. 2, 3).
Dilation of an autograft after the Ross procedure in late survivors has been reported from several studies.1, 2, 4) The reason for autograft aneurysm after the Ross procedure has not been clear yet; however, de Sa et al. have found histological malformation both in the ascending aorta and the pulmonary artery in the patients with bicuspid aortic valve disease. In fact, 75% of bicuspid aortic valve patients also had degenerative changes in pulmonary trunk.5) In our case, even we did not obtain pathological specimen, the degenerative changes in the aorta and pulmonary artery might have mediated aneurysmal changes, considering that both autograft and ascending aorta were aneurysmal.
The aortic root fixation using Dacron felt is applied to reinforce aortic annulus at the Ross procedure, and seemed very effective for this patient since no enlargement of aortic annulus and only mild autograft regurgitation were observed after 20 years. In fact, Fullerton et al.3) reported excellent midterm result using a felt to externally support the aortic annulus. In his report, of 44 patients, there were 3 early hospital deaths, no late death, no autograft aneurysm and only 1 reoperation due to recurrent endocarditis.
On the other hand, this technique may be ineffective to prevent autograft sinus of Valsalva aneurysm as seen in our case. Unsupported distal portion of the autograft still carries a risk of further dilation. Recently, in order to resolve autograft aneurysm, modified Ross procedure was proposed for adult patients.6, 7) In this procedure, the autograft was completely placed inside a Dacron graft for reinforcement. It is controversial whether young patients are good candidates for this procedure since autograft growth cannot be expected. Nevertheless, short and mid-term results are sufficient with no autograft aneurysm, and long-term result is awaited with interest.
In general, as previous studies have shown, results of reoperations for failed autografts were satisfactory; all-cause mortality of 0%.1) Even though there has been limited number of reports about repairing autograft aneurysm with Yacoub technique, Luciani and Ruzmetov et al.8, 9) had reported favorable long-term result of valve-sparing aortic root replacement with David and Yacoub techniques for autograft aneurysm.
In a case of autograft aneurysm with both annulus and sinus of Valsalva dilation, David technique is theoretically optimal for valve-sparing aortic root replacement, considering that Yacoub technique is incapable of stabilizing the autograft annulus. Nonetheless, under the Ross procedure with aortic annulus fixation, Yacoub technique may have several advantages including preservation of Valsalva configuration and minimum dissection of adhesions around the autograft and Dacron felt.10)
We present a case of autograft aneurysm repaired with valve-sparing root replacement. Further studies involving more patients are needed. However, under the Ross procedure with aortic annulus fixation, Yacoub technique for autograft aneurysm could be one of the choices.
Conflicts of Interest
All authors have no conflict of interest.
引用文献References
1) David TE, Ouzounian M, David CM, et al: Late results of the Ross procedure. J Thorac Cardiovasc Surg 2019; 157: 201–208
2) Luciani GB, Casali G, Favaro A, et al: Fate of the aortic root late after Ross operation. Ann Thorac Surg 2014; 98: 112–118
3) Fullerton DA, Fredericksen JW, Sundaresan RS, et al: The Ross procedure in adults: Intermediate-term results. Ann Thorac Surg 2003; 76: 471–476
4) Kalfa D, Magruder JT, Kalavrouziotis D, et al: Long-term outcomes of the Ross procedure in adults with severe aortic stenosis: Single-centre experience with 20 years of follow-up. Eur J Cardiothorac Surg 2015; 47: 159–167
5) de Sa M, Moshkovitz Y, Butany J, et al: Histologic abnormalities of the ascending aorta and pulmonary truink in patients with bicuspid aortic valve disease: Clinical relevance to the Ross procedure. J Thorac Cardiovasc Surg 1999; 118: 588–594
6) Juthier F, Banfi C, Vincentelli A, et al: Modified Ross operation with reinforcement of the pulmonary autograft: Six-year results. J Thorac Cardiovasc Surg 2010; 139: 1420–1423
7) Ungerleider RM, Ootaki Y, Shen I, et al: Modified Ross procedure to prevent autograft dilatation. Ann Thorac Surg 2010; 90: 1035–1037
8) Luciani GB, Lucchese G, Rita F, et al: Reparative surgery of the pulmonary autograft: Experience with Ross reoperations. Eur J Cardiothorac Surg 2012; 41: 1309–1315
9) Ruzmetov M, Welke KF, Geiss DM, et al: Failed autograft after the Ross procedure in children: Management and outcome. Ann Thorac Surg 2014; 98: 112–118
10) Lansac E, Centa I, Vojacek J, et al: Valve sparing root replacement: The remodeling technique with external ring annuloplasty. Ann Cardiothorac Surg 2013; 2: 117–123