Tetralogy of Fallot Repair: Surgical Approach to RVOTO
Pediatric Heart Institute, Hospital Universitario “12 de Octubre” ◇ Madrid, Spain
発行日:2017年7月1日Published: July 1, 2017
Repair of Tetralogy of Fallot is a challenging operation because of the high variability in the morphology of the right ventricular outflow tract and pulmonary valve (RVOT-PV) and the surgical technique that it entails. This review was prepared for pediatric cardiac surgeons with the objective of describing our approach on the correct assessment and operative technique for the repair of Tetralogy of Fallot based on a given RVOT-PV anatomy. A novel morphologic classification based on the RVOT-PV complex was provided.
Key words: tetralogy of fallot; pediatric cardiac surgery; surgical training; morphologic classification; operative tool
© 2017 特定非営利活動法人日本小児循環器学会© 2017 Japanese Society of Pediatric Cardiology and Cardiac Surgery
Repair of Tetralogy of Fallot (TOF) is a challenging operation because of the high variability of the right ventricular outflow tract and pulmonary valve (RVOT-PV) morphology and the consequent variable surgical technique to be used for its repair. The choice of an appropriate management of the RVOT-PV complex (e.g., whether or not to open the right ventricle (RV), placement of a transannular patch, preservation of the pulmonary valve (PV), etc.) can be difficult. In addition, an important degree of experience as pediatric cardiac surgeon is needed in order to perform the right operation for a given patient.
The objective of this review was to provide young pediatric cardiac surgeons with an operative tool to correctly assess and repair a TOF. Emphasis was placed on the surgical approach to relieve infundibular obstruction, so that unnecessary reoperations or ventriculotomies can be avoided. A morphologic classification based on the RVOT-PV complex was provided in the same way that truncus arteriosus and other pathologies are classified.
Relief of the infundibular obstruction may be pursued either by combined transatrial and transpulmonary approaches or through a right ventriculotomy. As for the ventricular septal defect (VSD), the approach for its closure has always been transatrial through the tricuspid valve. Relief of a right ventricular outflow tract obstruction (RVOTO) that is caused by mild or moderate hypertrophy of muscular bands can be usually achieved without the need for an infundibular incision.1, 2) The pulmonary valve can be normally preserved, but when its leaflets are severely dysplastic, regardless of the annulus Z-score, this conservative approach might not be successful. For borderline cases, a minimal incision on the pulmonary annulus (the “infundibular-sparing transannular patch method”) is needed. In the last few years, intraoperative balloon dilatation of the pulmonary annulus has emerged as an alternative technique for this subset of patients.1–5) When an RVOTO is caused by a hypoplastic infundibulum or severe muscle hypertrophy, relief is normally achieved through a right ventriculotomy, which allows patch enlargement with limited muscular resection.6) Often, the pulmonary annulus needs to be completely incised. Even in such cases, pulmonary regurgitation can be avoided by more aggressive techniques to reconstruct the valvular structure using custom-made monocusps, leaflet extensions, etc.7–10)
We classified TOF patients based on the anatomy of the RVOT-PV complex, in such a way that for a given type of TOF, a specific operative strategy can be suggested to address the RVOTO (Fig. 1). Of course, these recommendations are not absolute and the operative strategy in borderline cases may vary. Furthermore, different specific techniques, such as balloon annular dilatation, minimal annular incisions, and placement of mono-, bi-, or tricuspid valves may be applied in the same strategy.
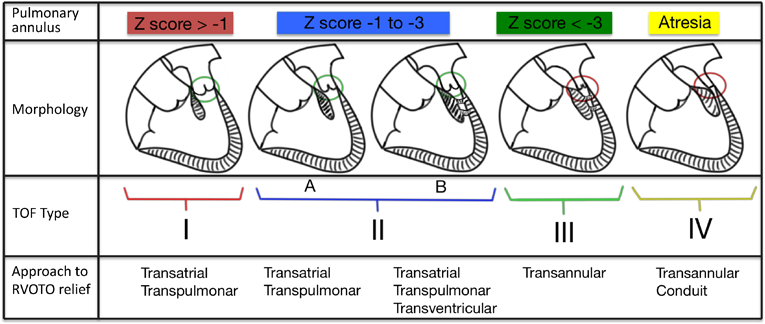
This is the so called “pink Fallot,” wherein the pulmonary annulus is normal or near-normal and the infundibular component of these RVOT-PV obstruction is absent or mild. A patient with TOF type I may present with minimal symptoms of heart failure or may be completely asymptomatic, such as in situations with balanced systemic and pulmonary total resistance and no significant shunt through the VSD.
This category includes patients with pulmonary annulus Z scores between −1 and −3. In this group, there is a high variability of the infundibular obstruction, which may be due to infundibular hypertrophy or hypoplasia. These patients present with different and changing degrees of cyanosis.
When the obstruction is due to mild or moderate hypertrophy of the infundibulum, which usually corresponds to a dynamic echocardiography gradient of ≤50% of the total, the TOF is classified as type IIa. On the other hand, when the obstruction is due to hypoplasia or severe hypertrophy of the infundibulum, which usually corresponds to a dynamic echocardiography gradient of >50% of the total, the TOF is classified as type IIb.
Patients in this category have a severely hypoplastic pulmonary annulus, with a Z score less than −3. Accordingly, the infundibulum is usually hypoplastic or severely hypertrophic. Symptoms related to severe cyanosis are frequent and some patients need urgent neonatal interventions, such as early total repair or any kind of palliation.
This group corresponds to TOF patients with pulmonary atresia and a ductus-dependent pulmonary circulation. Patients with MAPCAs are excluded from this classification. These patients constantly need a neonatal palliation to stabilize the pulmonary blood flow.
From a surgical point of view, these two groups of patients go together. Complete repair of the pathology may be accomplished transatrially and transpulmonary without any incision on the ventricular wall; the pulmonary valve function can often be preserved.
The relief of RVOT-PV obstruction is carried out through incisions in the atrium (i.e., muscular bands resection) and the pulmonary trunk (i.e., PV commissurotomy). Depending on the pulmonary artery (PA) trunk diameter, an augmentation patch for its closure may be needed. The patch can be made from fresh or glutaraldehyde-treated autologous pericardium or from a heterologous material.
In type IIa borderline cases with the pulmonary annulus Z score values in the −3 area, a small annular incision may be performed with or without pulmonary valve reconstruction (“infundibular-sparing transannular patch”); intraoperative balloon annular dilatation could be employed.1–5)
This group may be the most challenging to correctly define because these cases can be easily misclassified as type III, which requires a quite different surgical option than that in TOF type II. In fact, in type IIb patients, the infundibulum nearly always has to be incised and augmented with patch (ventriculotomy).6) But unlike it happens in patients with TOF type III, a transannular patch can be avoided in most cases, given that the Z score for the pulmonary annulus is greater than −3 (Fig. 2).
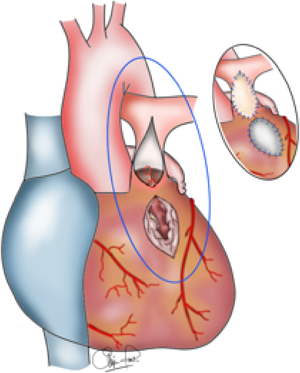
Two separate patches in the infundibulum and pulmonary trunk (plus pulmonary valve commissurotomy) are placed. The pulmonary annulus is preserved.
Unfortunately, the strategy described above does not automatically mean that valve function can be preserved in most patients. The pulmonary valve in this group is often very dysplastic, has poor leaflet mobility, and has a smaller effective orifice than the annular one; accordingly, the pulmonary trunk is often small. In a certain number of cases, the leaflets must be partially or totally resected, leaving a variable degree of pulmonary regurgitation that is usually less important than the one we get when the annulus is enlarged up to a normal Z score value.
As described for type IIa patients, if the Z score for the pulmonary annulus is in the −3 area, the same techniques of conservatively improving the annular diameter may be employed.1–5)
These patients almost invariably require a transannular patch for the relief of RVOT-PV obstruction. The classic technique of non-valve patching is still being used nowadays, although the length of the ventricular extension of the incision has been significantly reduced over the last decades. Nevertheless, this incision has to pass through the level of the most apical extension of the conal septum in order to reduce the risk of significant residual obstruction in the proximal infundibulum (Fig. 3a). On the other hand, the width of the patch at the annular level has to match a Z score of slightly less than 0 in order to reduce the magnitude of the pulmonary regurgitation. The consequences of the free pulmonary regurgitation derived from these techniques are well known and will invariably require pulmonary valvulation, either surgical or percutaneous, later on.11, 12)
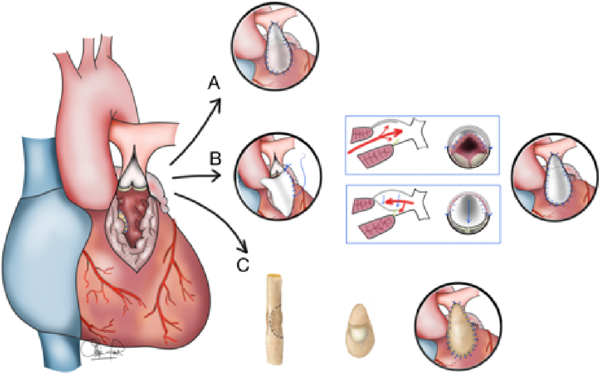
A transannular patch is almost always needed. The types of patch are a) the classic non-valved patch, b) a custom-made monocusp transannular patch, and c) a monocusp transannular patch derived from a valved bovine jugular vein conduit.
An alternative technique is the monocusp transannular patch, which aims to eliminate or at least reduce the amount of pulmonary regurgitation. The monocusp may be custom-made13–15) (Fig. 3b), using different materials, such as autologous pericardium, heterologous pericardium, other biological materials, or synthetic membranes; or can be derived from a segment of bovine jugular vein which contains one leaflet16) (Fig. 3c).
Patients with pulmonary atresia always need neonatal intervention to stabilize pulmonary blood flow. This may be done through a surgically created systemic to pulmonary shunt or an equivalent surgical palliation using a transannular patch with the VSD left open, or through a percutaneously delivered ductal stent. As an alternative, the patency of the ductus may be maintained by continuous prostaglandin infusion for a few weeks, followed by early complete repair.
At the time of TOF repair, usually within the first 3 to 6 months after the initial palliation, a conduit is used to reconstruct the continuity of the RVOT-PA. In a minority of patients, the caliber of the pulmonary trunk and the annulus, although small, allows their longitudinal opening and placement of a transannular patch, as in TOF type III patients.17, 18)
This review aimed to be an operative tool for the young cardiac surgeon who is facing his or her first cases of TOF repair as an independent operator. When attempting TOF repair, an inexperienced surgeon may have two opposite attitudes; they can be either too aggressive in infundibular/annular preservation or have a very low threshold for placing a transannular patch. In the first scenario, an intraoperative echocardiogram will show the residual obstruction, which can be relieved by a second pump run and aortic cross-clamping. In the second situation, a patient might undergo an aggressive operation that could have been avoided. Our algorithm could provide each patient the opportunity to receive the most appropriate and less invasive operation.
The authors have no conflicts of interest to declare.
1) Bové T, François K, Van De Kerckhove K, et al: Assessment of a right-ventricular infundibulum-sparing approach in transatrial-transpulmonary repair of tetralogy of Fallot. Eur J Cardiothorac Surg 2012; 41: 126–133
2) Padalino MA, Vida VL, Stellin G: Transatrial-transpulmonary repair of tetralogy of Fallot. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2009; 12: 48–53
3) Bacha E: Valve-sparing or valve reconstruction options in Tetralogy of Fallot surgery. Thorac Cardiovasc Surg Pediatr Card Surg Annu 2017; 20: 79–83
4) Vida VL, Guariento A, Zucchetta F, et al: Preservation of the pulmonary valve during early repair of tetralogy of Fallot: Surgical techniques. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2016; 19: 75–81
5) Robinson JD, Rathod RH, Brown DW, et al: The evolving role of intraoperative balloon pulmonary valvuloplasty in valve-sparing repair of tetralogy of Fallot. J Thorac Cardiovasc Surg 2011; 142: 1367–1373
6) Jonas RA: Early primary repair of Tetralogy of Fallot. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2009; 12: 39–47
7) Sung SC, Kim S, Woo JS, et al: Pulmonic valve annular enlargement with valve repair in tetralogy of Fallot. Ann Thorac Surg 2003; 75: 303–305
8) Anagnostopoulos P, Azakie A, Natarajan S, et al: Pulmonary valve cusp augmentation with autologous pericardium may improve early outcome for tetralogy of Fallot. J Thorac Cardiovasc Surg 2007; 133: 640–647
9) Sen DG, Najjar M, Yimaz B, et al: Aiming to preserve pulmonary valve function in tetralogy of Fallot repair: Comparing a new approach to traditional management. Pediatr Cardiol 2016; 37: 818–825
10) Stewart R, Backer CL, Young L, et al: Tetralogy of Fallot: Results of pulmonary valve sparing strategy. Ann Thorac Surg 2005; 80: 1431–1439, discussion, 1438–1439
11) Cullen S, Shore D, Redington AN: Characterization of right ventricular diastolic performance after complete repair of tetralogy of Fallot: Restrictive physiology predicts slow postoperative recovery. Circulation 1995; 91: 1782–1789
12) Kim H, Sung SC, Kim SH, et al: Early and late outcomes of total repair of tetralogy of Fallot: Risk factors for late right ventricular dilatation. Interact Cardiovasc Thorac Surg 2013; 17: 956–962
13) Hiramatsu Y: Pulmonary cusp and annular extension technique for reconstruction of right ventricular outflow in tetralogy of Fallot. Ann Thorac Surg 2014; 98: 1850–1852
14) Kumar M, Turrentine MW, Rodefeld MD, et al: Right ventricular outflow tract reconstruction with a polytetrafluoroethylene monocusp valve: A 20-Year experience. Semin Thorac Cardiovasc Surg 2016; 28: 463–470
15) Lee C, Lee CH, Kwak JG: Polytetrafluoroethylene bicuspid pulmonary valve replacement: A 5-year experience in 119 patients with congenital heart disease. Ann Thorac Surg 2016; 102: 163–169
16) Chiappini B, Barrea C, Rubay J: Right ventricular outflow tract reconstruction with contegra monocuspid transannular patch in tetralogy of Fallot. Ann Thorac Surg 2007; 83: 185–187
17) Kaza AK, Lim HG, Dibardino DJ, et al: Long-term results of right ventricular outflow tract reconstruction in neonatal cardiac surgery: Options and outcomes. J Thorac Cardiovasc Surg 2009; 138: 911–916
18) Cho JM, Puga FJ, Danielson GK, et al: Early and long-term results of the surgical treatment of tetralogy of Fallot with pulmonary atresia, with or without major aortopulmonary collateral arteries. J Thorac Cardiovasc Surg 2002; 124: 70–81
This page was created on 2017-05-31T17:10:44.619+09:00
This page was last modified on 2017-07-03T20:18:43.267+09:00
このサイトは(株)国際文献社によって運用されています。
