Percutaneous Pulmonary Valve Implantation: Lessons We Have Learned
Department of Pediatric Cardiology and Congenital Heart Defects, German Heart Centre Munich, Technical University Munich ◇ Germany
発行日:2018年3月31日Published: March 31, 2018
Percutaneous pulmonary valve implantation (PPVI), introduced two years before transcutaneous aortic valve implantation (TAVI) is one of the most successful recent improvements in catheter interventional treatment of patients with congenital heart disease and dysfunction of the right ventricular outflow tract (RVOT). At adolescence, many patients with complex cardiac lesions involving the RVOT have experienced several open heart surgeries. Repeated open heart operations are associated with significant morbidity and even mortality. The Melody® valve was initially introduced to expand the life time of a biological valve in the RVOT and hence to reduce the total number of open heart surgeries during a patients life time. The advent of the Sapien® valve now enables treatment of RVOT’s as large as 31 mm in diameter and even patients with so called “native” right ventricular outflow tracts (without a biological valved conduit) are amenable to treatment with a percutaneous valve. PPVI is safe and effective and patients can be discharged home after a few days in the hospital. Coronary occlusion and conduit rupture are the major hazards of the intervention. Long-term data on valve durability now show similar results in comparison to surgical valve implantation with less morbidity for the patients. Currently new self expanding valves are tested, which could enhance the possibility for patient selection. This review describes current practice, adds own experience, lessons learned and gives an outline on future developments in PPVI.
Key words: percutaneous pulmonary valve implantation; right ventricular outflow tract dysfuncion
© 2018 特定非営利活動法人日本小児循環器学会© 2018 Japanese Society of Pediatric Cardiology and Cardiac Surgery
The incidence of congenital heart disease (CHD) varies between 4 and 8 per 1000 live birth.1, 2) Patients with Tetralogy of Fallot, common arterial trunc, pulmonary atresia and ventricular septal defect, transposition of the great arteries after Rastelli operation and patients with valvar aortic stenosis after the Ross procedure require complex cardiothoracic operations, often at infant age, involving the right ventricular outflow tract (RVOT). Today, up to 90% of these patients survive to adulthood.3) However, RVOT dysfunction is a common finding in the above mentioned patients and pulmonary valve replacement with a biological valve may be necessary. The longevity of biological valves is limited and in the past subsequent repeated surgical pulmonary valve exchanges were necessary.4) At present, RVOT conduit revision can be performed with a very low mortality,5–7) but repeated redo operations are associated with significant morbidity8) and the technical challenge rises with the number of re-operations.
Percutaneous pulmonary valve implantation (PPVI) was introduced as the first successful catheter interventional valve implantation in the year 20009) and is one of the most significant advances in catheter interventional treatment of patient with CHD in the last decades. PPVI ermerged to the preferred first line treatment for selected patients with RVOT dysfunction in many centres. The idea of Philip Bonhoeffer was to prolong the functional life-span of a biological valve prosthesis in the RVOT with the final goal to reduce the total number of open heart surgeries required over a patient’s lifetime. So far, several studies documented excellent immediate and medium term hemodynamic results after PPVI with the Melody valve (Medtronic, Minneapolis, MN, USA)10–15) and with the Sapien valve (Edwards, Irvine, CA, USA)16, 17) in pulmonic position. Worldwide more than 11.000 PPVI procedures have been performed. The melody valve received the CE mark for Canada and Europe in 2006 and received FDA use approval in 2010. The Sapien XT valve was approved by the FDA for percutaneous implantation in pulmonic position in the year 2016.
A biological valve in the RVOT has a limited life-span. Due to valve degeneration or outgrowth even adult sized valves (>18 mm diameter) have to be exchanged at mean after 10–15 years.4) Current guidelines for surgical pulmonary valve replacement evenly apply for PPVI as well (Table 1).18–20)
| The following situations may warrant intervention following repair: |
| — Free pulmonary regurgitation associated with: |
| ◦ Progressive or moderate to severe RV enlargement (RV end-diastolic volume of greater than 170 mL/m2) |
| ◦ Moderate to severe RV dysfuntion |
| ◦ Important tricuspid regurgitation |
| ◦ Atrial or ventricular arrhythmias |
| ◦ Symptoms such as deteriorating exercise performance |
| European Society of Cardiology guidelines for surgical PVR19): |
| — PVR should be performed in symptomatic patients with severe PR and/or stenosis (RV systolic pressure >60 mmHg, TR velocity >3,5 m/s) |
| — PVR should be considered in asymptomatic pateints with severe PR and/or stenosis when at least one of the following criteria is present: |
| ◦ Decrease in objective exercise capacity |
| ◦ Progressive RV dilatataion |
| ◦ Progressive RV sytolic dysfunction |
| ◦ Progressive TR (at least moderate) |
| ◦ RVOT with systolic pressure >80 mmHg (TR velocity >4,3 m/s) |
| ◦ Sustained atrial/ventricular arrhythmias |
| PR: Pulmonary regurgitation, PS: Pulmonary stenosis, PVR: Pulmonary valve replacement, RVOT: Right ventricular outflow tract. |
The pre procedural work-up always includes a patient history, detailed reports of former operations (which valve is in place?), a clinical examination, an echocardiographic examination, a cardiovascular magnetic resonance tomography and an exercise test with assessment of VO2 max. At present these examinations are repeated at 6 months, five and ten years after PPVI at our unit. Since large sheaths are necessary for PPVI the femoral or jugular vessels have to be large enough to accommodate an introducer sheath for the specific valve 22F.
Our approach—We recommend percutaneous pulmonary valve implantation for patients with right ventricle to pulmonary artery conduits, native right ventricular outflow tracts (“off label” indication), or failing bioprosthetic valves in the pulmonary position meeting the following criteria for severe RVOT obstruction or severe pulmonic regurgitation (Table 2). Most patients show a combination of stenosis and regurgitation in the RVOT.
| — Severe RVOT obstruction with no or mild pulmonary regurgitation, with either of the following: |
| ◦ Symptoms related to RVOT obstruction (<65% of expected or a significant decrease in exercise tolerance) plus a peak Doppler velocity at the tricuspid valve >3,5 m/s or |
| ◦ No symptoms plus an increased RV pressure >4,3 m/s (measured at tricuspid regurgitation),>2/3 systemic pressure in the right ventricle |
| — Severe pulmonary regurgitation, with right ventricular end-diastolic volume index >150 mL/m2 by cardiovascular magnetic resonance imaging21) |
| Candidates for PPVI must also meet the following criteria: |
| — Adequate RVOT conduit size to accommodate a covered stent. We do not have a lower size limitation. The upper size limitation is usually a diameter >29 mm. In selected cases, a patient with a slightly larger RVOT diameter may be successfully treated after prestenting to a smaller diameter, or by overfilling the dilatation balloon (Sapien S3 29 may be overdilated to 31 mm outer diameter). |
| — Adequate body size. There is no absolute lower age limit but an adequate body size (eg, weight >20 kg) is required to accommodate femoral placement of the introducer. |
| PPVI: Percutaneous pulmonary valve implantation, RVOT: Right ventricular outflow tract |
PPVI is not possible, if there is occlusion of all central veins, active infection (such as infective endocarditis) or high risk of infection, or if the “balloon test” show severe proximity of a coronary vessel to the RVOT landing zone.22)
The intervention is carried out in general anaesthesia, or in deep conscious sedation. After vascular access is achieved for both the femoral vein and artery a complete diagnostic catheterization is performed. If femoral veins are occluded, a jugular venous access may be used. A weight adjusted dose of heparin (100 units/kg, max. 5,000 units) is given. The gradient between the right ventricle (RV) and the pulmonary artery is assessed and the systolic pressure ratio between the aorta and the RV is calculated. An angiogram into the RVOT defines the dimensions and according to the measured diameters a balloon test with a concomitant aortogram is performed to depict the anatomy of the RVOT in relation to the coronary arterial system.22) If the coronary anatomy is doubtful a balloon test with a high pressure balloon (Atlas gold Bard, Tempe, AZ, USA) through a 14F long sheath and selective injections into the coronary arteries in different X-ray planes may be necessary. It is safer to perform the high pressure dilatation through a long sheath, because RVOT rupture can rapidly be depicted by dyse injections through the sheath and once the rupture has occurred a covered stent can then rapidly be delivered through the long sheath. Then a pre-stent is implanted with a balloon catheter into the RVOT landing zone over a superstiff guide wire (Amplatz ultrastiff, Lunderquist, Meier wire), which had been placed distally into one pulmonary artery. In calcified RVOT’s we prefer the use of a covered stent (for example a covered CP-stent NuMED, Inc. Hopkinton, NY, USA). If stent-recoil is visible during balloon dilation the implantation of additional stents (bare metal stents) may be indicated and the prepared landing zone is dilated with high pressure balloons to the desired final internal diameter. Depending on the patient’s age, weight and the anatomical situation, the largest possible internal diameter of the landing zone should be achieved to have the best possible hemodynamic result. An appropriately sized pulmonic valve (Melody or Sapien valve) is prepared and implanted over the guide wire. The pressure recordings are repeated and final angiograms document correct valve position and intact vessels. The intervention is successful if the post interventional gradient between the subpulmonary ventricle and the pulmonary arteries is <20 mmHg. Whenever the gradient exceeds this value, high pressure balloon dilatation may be necessary to acieve a better result.
The Medtronic Melody® valve (Fig. 1) system involves a balloon-expandable prosthesis that is available in two sizes, 16 and 18 mm, suited for RVOT dimensions from 16–24 mm. The bovine jugular vein is sutured into a bare metal 34 mm 8 zig Cheatham platinum stent (Cheatham Platinum stent, NuMED Inc., Hopkinton, NY). Expanded to 22 mm internal diameter the stent shortenes to a length of 24 mm. The valve is hand crimped onto a 18, 20 or 22 mm balloon-in-balloon delivery catheter (Ensemble Transcatheter Delivery System, Minneapolis, MN, USA) with a maximal outer diameter of 22F. The delivery system is then closed over the valve and the ensemble is guided over the wire into the final landing zone, where it can be re-opened, after which the BiB balloons are inflated. The 16 mm Melody® valve can only be expanded to a maximum of 20 mm internal diameter.

It can expanded to 24 mm external diameter with a 22 mm Ensemble® Delivery System. The length of the Melody® Transcatheter Pulmonary Valve varies between 26.2, 24.2 or 23 mm respectively, depending upon the size of the Ensemble® Delivery System used (18, 20, 22 mm, respectively, Medtronic Inc. Minneapolis, MN). The smaller 16 mm valve can only be expanded to 20 mm internal diameter.
The Edwards Sapien® valve (Fig. 2) is a trileaflet bovine pericardial valve, hand sutured onto a rigid chromium-cobalt stent frame and is available in four sizes, 20 mm, 23 mm, 26 mm and 29 mm external diameter. Once dilated the stent length ranges from 14.3 mm for the 23 mm valve to 19.1 mm for the 29 mm valve. The valve is crimped using a specially designed tool to mount it onto a 30 mm long, noncompliant high pressure balloon. The valve is delivered through a 14 or 16F sheath into the femoral vein. The French size refers to the internal diameter of the expandable sheaths. The outer diameter of the Melody® valve is 22F, but it can be delivered through the Edwards 16F e-sheath. Hence, the external diameters of the valves (Melody® and Sapien® 23, 26, 29) do not differ significantly. Once in the inferior vena cava the valve is pushed forward onto the balloon. It is then advanced unguarded through the tricuspid valve into the final landing zone in the RVOT over the guide wire, where the valve is balloon dilated.
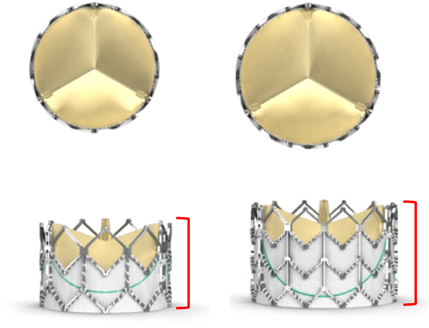
The length of the expanded Sapien 26 mm valve is 17.2 mm and of the Sapien 29 mm valve is 19.1 mm. The valve is available in 23, 26 and 29 mm external diameters.
Three prospective studies in the US, Canada and Europe documented excellent immediate procedural results with the Melody® valve, which persist to medium term follow-up.23–26) These studies report on a high incidence of successful valve implantations with a significant RVOT gradient reduction, sustained abolishment of pulmonary regurgitation, a low incidence of procedural adverse events and low rate of adverse device related events. The same, with smaller patient numbers and shorter follow-up, is published for the Sapien® valve in pulmonic position.17)
The incidence of major life threatening procedural complications is very low (< 1%). However, there are two possible major procedure related complications. Coronary compression caused by the stents of the valve or the prestents may occur resulting in acute myocardial ischemia. The balloon test was suggested to rule out possible coronary compression.22) In one multicenter study 5% of all patients showed signs of coronary compression during a balloon test.27) On the other hand a balloon test, especially with a high pressure balloon, may lead to conduit rupture.28, 29) In case of a non-contained RVOT rupture, covered stents must be available to control this dangerous and potentially fatal complication. If catheter interventional means are not successful, a skilled surgical team may be able to save the life of the patient in this dramatic situation.30)
In the initial Melody® patient group, a stent fracture rate of 21% was reported and a classification of stent fractures after PPVI was developed.31) Pre-stenting and meticulous preparation of the RVOT landing zone reduced the incidence of clinically significant stent fractures of the Melody® valve.11, 32, 33)
Infective endocarditis (IE) is a potential late complication associated with all types of bioprosthetic valve implants no matter if the valve is implanted surgically, or by percutaneous means. The original Duke criteria to diagnose IE were introduced by Durack et al. in 199434) and later modified by Li et al.35) The Duke criteria were developed for native valve IE and do not apply for patients after prosthetic valve implantation. Hence, it may be very difficult or impossible to visualize the valve leaflets using regular echocardiographic means due to multiple artefacts. PET-CT, SPECT and intracardiac echocardiography were suggested as additional diagnostic tools to diagnose valve related IE.36–38) Estimates of its incidence after PPVI with the Melody valve vary widely with a general range from 2.5–4% per patient year.39–41) Combined results of 3 prospective North American, Canadian and European studies identified an annualized rate of a first episode of IE of a Melody® valve at 2.4% per patient year. The proven valve related rate of IE was 0.88% per patient year for the Melody® valve.42) Risk factors include unprotected dental treatment, male gender, multiple stents, aspirin non-complicance and a previous history of IE.39–42) The risk of IE appears to be higher in patients who undergo Melody® valve implantation compared to surgical pulmonary valve replacement.40) However, no prospectively examined comparison between surgery and PPVI is yet available. IE after PPVI can be effectively managed with antibiotics, though severe cases may require instant surgical explantation of the valve,42) or a palliative bare metal stent implantation for relief of severe RVOT obstruction.
One group postulates an enhanced selective adhesion of S. aureus and S. sanguinis pathogenic strains to Melody® valve tissue after balloon dilatation of the valve tissue.43) Hence, tissue micro lacerations may occur at high pressure ballooning of the bovine valve, which may be a cite for early thrombus formation. Other experimental evidence showed that the surface composition of bovine jugular valves and homograft tissue themselves, bacterial surface proteins, and shear forces per se are not the prime determinants of bacterial adherence.44) Finally, one group proposes that the risk for IE is lower after PPVI with a Sapien® valve compared to the Melody® valve.45) At present this question is still open and more solid information is required for a definite answer.
Contemporary data suggests that in patients after PPVI, rates of freedom from re-intervention are greater than 90% at 1 year, down to 76% at 5 years in patients without stent fracture.46) Risk factors for re-intervention include the presence of a homograft,no pre-stenting, post PPVI RVOT gradient greater than 25 mmHg, and a pre-implantation moderate-to-severe tricuspid regurgitation.10, 46) However, it was demonstrated that PPVI had a positive effect on RV remodeling, even in the presence of moderate to severe tricuspid regurgitation.47, 48) Patients with RVOT dysfunction (stenosis, regurgitation or both) show an improved exercise capacity after PPVI.49) Finally, in current practice, survival is approximately 98% at 5 years and 97% at 7 years.10, 46)
In our own experience of 240 patients after PPVI the incidence of IE was 2.0% per patient year and 91% of our patients still live with their first percutaneously implanted valve.50)
Percutaneous pulmonary valve implantation with the Melody® and Sapien® valves equally proved to be safe, effective and with sustained improvement of the hemodynamics, the exercise capacity and the functional class of the patients. Hence, PPVI is one of the major advances of catheter interventional treatment of patients with CHD and RVOT dysfunction in the last two decades. This method appears similar in terms of suspected long-term outcomes to open heart surgery, though further data are necessary to prove this.
However, today not all patients with RVOT dysfunction are amenable to PPVI. The largest external diameter of the currently available valves is 31 mm, if a Sapien® 29 valve is overdilated. A significant number of patients with large RVOT’s with treatment indication still need surgical pulmonary valve replacement.
To overcome this limitation, a self-expanding valve was developed and firstly implanted into a patient with a large RVOT and significant pulmonary regurgitation in the year 2009.51) Based on this experience the Harmony® valve (Medtronic, Minneapolis, MN, USA) a self-expanding porcine pericardial tissue valve with asymmetric hourglass configuration was developed. Recently, the results of the patients selection process and the six months outcomes after Harmony® implantation in the first 20 patients were published. Device implantation was safe, with a high procedural success rate.52, 53) Currently, further 40 patients are scheduled for treatment with this device under study conditions in North America.
The venous P® transcatheter valve system (Venus Medtech, Shanghai, China) is composed of a tri-leaflet porcine pericardial tissue valve, mounted on a self-expanding nitinol stent. To accommodate larger diameter conduits, the stent has proximal and distal flares to anchor the valve. The valve is crimped and loaded onto the delivery system, which is then advanced throught a 22–24F sheath. Valve sizes range from 20–32 mm diameter54) and the valve is implanted in Europe under study conditions.
Finally, the Altera® device (Edwards Lifesciences, Irvine, CA, USA) is a self-expanding covered nitinol stent (40×45 mm) which could serve as a rigid landing zone for the 29 mm Sapien valve. There is an ongoing clinical feasibility trial, approved by the FDA. Once all these technical innovations are clinically available more patients with RVOT dysfunction will be amenable to catheter interventional treatment.
Andreas Eicken is a proctor for the Medtronic Melody valve, and Peter Ewert is a proctor for the Medtronic Melody valve and for the Edwards Sapien valve.
1) Schwedler G, Lindinger A, Lange PE, et al: Frequency and spectrum of congenital heart defects among live births in germany: A study of the competence network for congenital heart defects. Clin Res Cardiol 2011; 100: 1111–1117
2) Ferencz CBJ, Neill CA, Brenner JI, et al: Congenital cardiovascular malformations: Questions on inheritance. Baltimore-washington infant study group. J Am Coll Cardiol 1989; 14: 756–763
3) Wren C, O’Sullivan JJ: Survival with congenital heart disease and need for follow up in adult life. Heart 2001; 85: 438–443
4) Homann M, Haenel JC, Mendler N, et al: Reconstruction of the rvot with valved biological conduits: 25 years experience with allografts and xenografts. Eur J Cardiothorac Surg 2000; 17: 624–630
5) Kanter KR, Budde JM, Parks WJ, et al: One hundred pulmonary valve replacements in children after relief of right ventricular outflow tract obstruction. Ann Thorac Surg 2002; 73: 1801–1806, discussion, 1806–1807
6) Lange R, Weipert J, Homann M, et al: Performance of allografts and xenografts for right ventricular outflow tract reconstruction. Ann Thorac Surg 2001; 71 Suppl: S365–S367
7) Khanna AD, Hill KD, Pasquali SK, et al: Benchmark outcomes for pulmonary valve replacement using the society of thoracic surgeons databases. Ann Thorac Surg 2015; 100: 138–146, discussion, 145–146
8) Dilber D, Hoerer J, Malčić I, et al: Percutaneous pulmonary valve implantation and surgical valve replacement in patients with right ventricular outflow tract dysfunction—A complementary treatment concept. Int J Cardiol 2013; 169: e3–e5
9) Bonhoeffer P, Boudjemline Y, Saliba Z, et al: Percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction. Lancet 2000; 356: 1403–1405
10) Lurz P, Coats L, Khambadkone S, et al: Percutaneous pulmonary valve implantation: Impact of evolving technology and learning curve on clinical outcome. Circulation 2008; 117: 1964–1972
11) Eicken A, Ewert P, Hager A, et al: Percutaneous pulmonary valve implantation: Two-centre experience with more than 100 patients. Eur Heart J 2011; 32: 1260–1265
12) Butera G, Milanesi O, Spadoni I, et al: Melody transcatheter pulmonary valve implantation. Results from the registry of the italian society of pediatric cardiology. Catheter Cardiovasc Interv 2013; 81: 310–316
13) McElhinney DB, Hellenbrand W, Zahn EM, et al: Short- and medium-term outcomes after transcatheter pulmonary valve placement in the expanded us medody trial. Circulation 2010; 122: 507–516
14) Cools B, Budts W, Heying R, et al: Medium term follow-up after percutaneous pulmonary valve replacement with the melody® valve. Int J Cardiol Heart Vasc 2015; 7: 92–97
15) Solana-Gracia R, Rueda F, Betrián P, et al: Pediatrics spanish registry of percutaneous melody pulmonary valve implantation in patients younger than 18 years. Rev Esp Cardiol (Engl Ed). 2017: 30435-30438. doi: 30410.31016/j.rec.32017.30407.30013. [Epub ahead of print] English, Spanish
16) Kenny D, Hijazi ZM, Kar S, et al: Percutaneous implantation of the edwards sapien transcatheter heart valve for conduit failure in the pulmonary position: Early phase 1 results from an international multicenter clinical trial. J Am Coll Cardiol 2011; 58: 2248–2256
17) Haas NA, Carere RG, Kretschmar O, et al: Early outcomes of percutaneous pulmonary valve implantation using the edwards sapien xt transcatheter heart valve system. Int J Cardiol 2017; pii: S0167-5273816934047-5
18) Silversides CK, Kiess M, Beauchesne L, et al: Canadian cardiovascular society 2009 consensus conference on the management of adults with congenital heart disease: Outflow tract obstruction, coarctation of the aorta, tetralogy of fallot, ebstein anomaly and marfan’s syndrome. Can J Cardiol 2010; 26: e80–e97
19) Baumgartner H, Bonhoeffer P, De Groot NM, et al: Task force on the management of grown-up congenital heart disease of the European Society of Cardiology (ESC); Association for European Paediatric Cardiology (AEPC); ESC Committee for Practice Guidelines (CPG): Esc guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J 2010; 31: 2915–2957
20) Feltes TF, Bacha E, Beekman RH 3rd, et al: American Heart Association Congenital Cardiac Defects Committee of the Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; American Heart Association: Indications for cardiac catheterization and intervention in pediatric cardiac disease: A scientific statement from the american heart association. Circulation 2011; 123: 2607–2652
21) Frigiola A, Tsang V, Bull C, et al: Biventricular response after pulmonary valve replacement for right ventricular outflow tract dysfunction: Is age a predictor of outcome? Circulation 2008; 118 Suppl: S182–S190
22) Sridharan S, Coats L, Khambadkone S, et al: Images in cardiovascular medicine. Transcatheter right ventricular outflow tract intervention: The risk to the coronary circulation. Circulation 2006; 113: e934–e935
23) McElhinney DB, Hellenbrand W, Zahn EM, et al: Short- and medium-term outcomes after transcatheter pulmonary valve placement in the expanded multicenter us melody valve trial. Circulation 2010; 122: 507–516
24) Armstrong AK, Balzer DT, Cabalka AK, et al: One-year follow-up of the melody transcatheter pulmonary valve multicenter post-approval study. JACC Cardiovasc Interv 2014; 7: 1254–1262
25) McElhinney DB, Cheatham JP, Jones TK, et al: Stent fracture, valve dysfunction, and right ventricular outflow tract reintervention after transcatheter pulmonary valve implantation: Patient-related and procedural risk factors in the us melody valve trial. Circ Cardiovasc Interv 2011; 4: 602–614
26) Hager A Schubert S, Ewert P, Søndergaard L, et al: Five-year results from a prospective multicentre study of percutaneous pulmonary valve implantation demonstrate sustained removal of significant pulmonary regurgitation, improved right ventricular outflow tract obstruction and improved quality of life. EuroIntervention 2017; 12: 1715–1723
27) Morray BH, McElhinney DB, Cheatham JP, et al: Risk of coronary artery compression among patients referred for transcatheter pulmonary valve implantation. Circ Cardiovasc Interv 2013; 6: 535–542
28) Boe BA, Bocks ML, Armstrong AK: Contained rupture of patched right ventricular outflow tracts during balloon sizing for percutaneous pulmonary valve implantation. Catheter Cardiovasc Interv 2016; 87: 768–772
29) Boudjemline Y, Malekzadeh-Milani S, Patel M, et al: Predictors and outcomes of right ventricular outflow tract conduit rupture during percutaneous pulmonary valve implantation: A multicentre study. EuroIntervention 2016; 11: 1053–1062
30) Kostolny M, Tsang V, Nordmeyer J, et al: Rescue surgery following percutaneous pulmonary valve implantation. Eur J Cardiothorac Surg 2008; 33: 607–612
31) Nordmeyer J, Khambadkone S, Coats L, et al: Risk stratification, systematic classification, and anticipatory management strategies for stent fracture after percutaneous pulmonary valve implantation. Circulation 2007; 115: 1392–1397
32) Nordmeyer J, Lurz P, Khambadkone S, et al: Pre-stenting with a bare metal stent before percutaneous pulmonary valve implantation: Acute and 1-year outcomes. Heart 2011; 97: 118–123
33) Cabalka AK, Hellenbrand W, Eicken A, et al: Relationships among conduit type, pre-stenting, and outcomes in patients undergoing transcatheter pulmonary valve replacement in the prospective north american and european melody valve trials. JACC Cardiovasc Interv 2017; 10: 1746–1759
34) Durack DT, Lukes AS, Bright DK; Duke Endocarditis Service: New criteria for diagnosis of infective endocarditis: Utilization of specific echocardiographic findings. Am J Med 1994; 96: 200–209
35) Li JS, Sexton DJ, Mick N, et al: Proposed modifications to the duke criteria fort he diagnosis of infective endocarditis. Clin Infect Dis 2000; 30: 633–638
36) Habib GLP, Antunes MJ, Bongiorni MG, et al: 2015 esc guidelines for the management of infective endocarditis: The task force for the management of infective endocarditis of the european society of cardiology (esc). Endorsed by: European association for cardio-thoracic surgery (eacts), the european association of nuclear medicine (eanm). Eur Heart J 2015; 36: 3075–3128
37) Cheung G, Vejlstrup N, Ihlemann N, et al: Infective endocarditis following percutaneous pulmonary valve replacement: Diagnostic challenges and application of intra-cardiac echocardiography. Int J Cardiol 2013; 169: 425–429
38) Salaun E, Sportouch L, Barral PA, et al: Diagnosis of infective endocarditis after tavr: Value of a multimodality imaging approach. JACC Cardiovasc Imaging 2017; pii: S1936-878X(17)30604-6. doi: 10.1016/j.jcmg.2017.05.016. [Epub ahead of print] No abstract available
39) Malekzadeh-Milani S, Ladouceur M, Patel M, et al: Incidence and predictors of melody® valve endocarditis: A prospective study. Arch Cardiovasc Dis 2015; 108: 97–106
40) Van Dijck I, Budts W, Cools B, et al: Infective endocarditis of a transcatheter pulmonary valve in comparison with surgical implants. Heart 2015; 101: 788–793
41) Buber J, Bergesen L, Lock JE, et al: Bloodstream infections occurring in patients with percutaneously implanted bioprosthetic pulmonary valve: A single-center experience. Circ Cardiovasc Interv 2013; 6: 301–310
42) McElhinney DB, Benson LN, Eicken A, et al: Infective endocarditis after transcatheter pulmonary valve replacement using the melody valve: Combined results of 3 prospective north american and european studies. Circ Cardiovasc Interv 2013; 6: 292–300
43) Jalal Z, Galmiche L, Lebeaux D, et al: Selective propensity of bovine jugular vein material to bacterial adhesions: An in-vitro study. Int J Cardiol 2015; 198: 201–205
44) Veloso TR, Claes J, Van Kerckhoven S, et al: Bacterial adherence to graft tissues in static and flow conditions. J Thorac Cardiovasc Surg 2017; 155: 325–332.e4 [(Epub ahead of print)] Medline
45) Hascoet S, Mauri L, Claude C, et al: Infective endocarditis risk after percutaneous pulmonary valve implantation with the melody and sapien valves. JACC Cardiovasc Interv 2017; 10: 510–517
46) Cheatham JP, Hellenbrand W, Zahn EM, et al: Clinical and hemodynamic outcomes up to 7 years after transcatheter pulmonary valve replacement in the us melody investigational device exemption trial. Circulation 2015; 131: 1960–1970
47) Tanase D, Ewert P, Georgiev S, et al: Tricuspid regurgitation does not impact right ventricular remodeling after percutaneous pulmonary valve implantation. JACC Cardiovasc Interv 2017; 10: 701–708
48) Jones TK, Rome JJ, Armstrong AK, et al: Transcatheter pulmonary valve replacement reduces tricuspid regurgitation in patients with right ventricular volume/pressure overload. J Am Coll Cardiol 2016; 68: 1525–1535
49) Müller J, Engelhardt A, Fratz S, et al: Improved exercise performance and quality of life after percutaneous pulmonary valve implantation. Int J Cardiol 2014; 173: 388–392
50) Tanase D, Ewert P, Hager A, et al: Infective endocarditis after percutaneous pulmonary valve implantation—Long-term single centre experience. Int J Cardiol 2018; Revision submitted
51) Schievano S, Taylor AM, Capelli C, et al: First-in-man implantation of a novel percutaneous valve: A new approach to medical device develpment. Eurintervention 2010; 5: 745–750
52) Bergersen L, Benson LN, Gillespie MJ, et al: Harmony feasibility trial: Acute and short-term outcomes with a self-expanding transcatheter pulmonary valve. JACC Cardiovasc Interv 2017; 10: 1763–1773
53) Gillespie MJ, Benson LN, Bergersen L, et al: Patient selection process for the harmony transcatheter pulmonary valve early feasibility study. Am J Cardiol 2017; 120: 1387–1392
54) Promphan W, Prachasilchai P, Siripornpitak S, et al: Percutaneous pulmonary valve implantation with the venus P-valve: Clinical experience and early results. Cardiol Young 2016; 26: 698–710
This page was created on 2018-03-28T13:11:57.022+09:00
This page was last modified on 2018-04-16T11:30:18.373+09:00
このサイトは(株)国際文献社によって運用されています。
