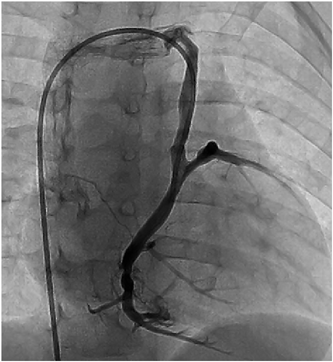
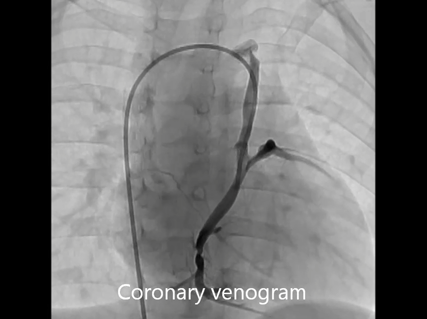
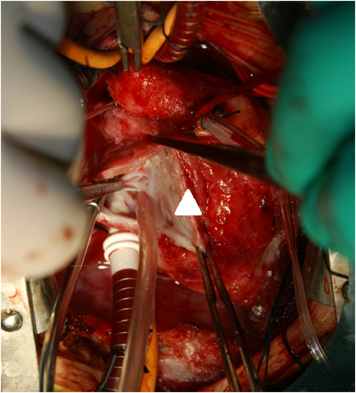
Coronary Sinus Orifice Atresia in Tricuspid Atresia
1 Department of Pediatrics, Japan Community Healthcare Organization Kyushu Hospital ◇ Fukuoka, Japan
2 Department of Cardiovascular Surgery, Japan Community Healthcare Organization Kyushu Hospital ◇ Fukuoka, Japan
受付日:2017年8月14日Received: August 14, 2017
受理日:2018年2月23日Accepted: February 23, 2018
発行日:2018年7月1日Published: July 1, 2018