Congenital heart disease is a risk factor for infective endocarditis. An aortic pseudoaneurysm is a rare but life-threatening complication associated with cardiac surgical procedures. Aortic dissection, infection, connective tissue disorders, chronic hypertension, aortic calcification, and aortotomy dehiscence are known factors that predispose individuals to aortic pseudoaneurysms.1) However, an aortic pseudoaneurysm in the ascending aorta after infective endocarditis of the aortic valve in children is rare.2) The treatment involves surgical intervention via procedures, such as patch aortoplasty, graft replacement, or aortic valve replacement. Here, we report a case involving a 10-year-old boy with congenital aortic valve stenosis who developed an ascending aortic pseudoaneurysm after infective endocarditis of the aortic valve.
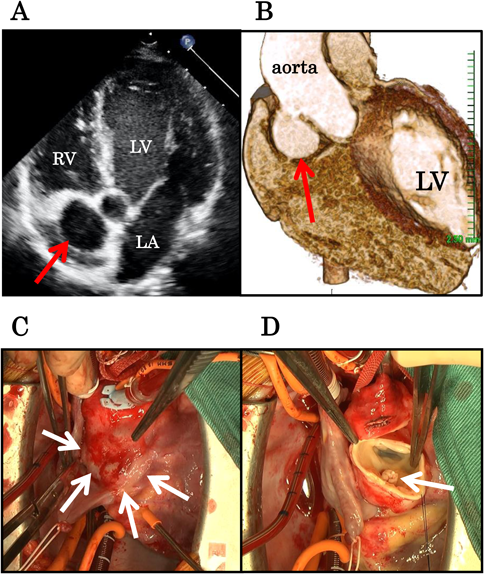
A 10-year-old boy was admitted to our hospital with fever of unknown origin. He had undergone percutaneous balloon aortic valvoplasty for congenital aortic valve stenosis when he was 2 years old. The initial pressure gradient at the aortic valve was 60 mmHg before valvoplasty. After percutaneous aortic valvoplasty, it decreased to 40 mmHg. The patient exhibited trivial aortic valve regurgitation. The balloon size was 95% of the aortic valve size. At the time of the current admission, his blood pressure was 100/60 mmHg; heart rate, 90 bpm; and respiratory rate, 16 breaths per minute. His body temperature was 38.0°C. Physical examination revealed a Levine-III/VI systolic-ejection murmur at the second right intercostal space. Laboratory investigations showed leukocytosis (14,000 cells/mm,3) 70% polymorphonuclear leukocytes), and his C-reactive protein level was elevated to 6.5 mg/dL. A chest radiograph showed no obvious signs of pneumonia or pulmonary congestion. Electrocardiography revealed sinus rhythm and no other abnormalities. The echocardiogram showed aortic valve stenosis, with a peak aortic pressure gradient of 40 mmHg. The parasternal long-axis view revealed vegetation attached to the aortic valve of the noncoronary cusp. We noted a thickened bicuspid aortic valve. Considering the size of vegetation, aortic valve stenosis was not caused by the vegetation. He was diagnosed with infective endocarditis of the aortic valve and treatment with aminobenzyl penicillin (200 mg/kg/day) for 6 weeks and intravenous gentamicin (3 mg/kg/day) for 2 weeks was initiated. Blood cultures obtained at the time of admission revealed the growth of Streptococcus mitis. After antibiotic administration, his body temperature returned to within the normal range 2 days after admission. However, echocardiography after antibiotic therapy showed an abnormal cavity near the ascending aorta (Fig. 1A). Although we performed echocardiography once per week during therapy, we did not detect the aneurysm until then. Contrast-enhanced computed tomography (CT) showed a defect in the right anterior wall of the ascending aorta, 5 mm above the aortic valve, and a pseudoaneurysm originating from the defect (Fig. 1B). Figures A and B are images obtained after 6 and 7 weeks of antibiotic treatment, respectively. The patient subsequently underwent ascending aortic replacement with a J graft (18 mm) to avoid rupturing the pseudoaneurysm 2 weeks after completing the antibiotic treatment. Intraoperative findings revealed a small amount of vegetation near the pseudoaneurysm entry-point (Fig. 1C, D); however, there was no sign of aortic valve infection. The postoperative course was uncomplicated, and the patient was discharged 4 weeks after the surgery.
A pseudoaneurysm in the ascending aorta after infective endocarditis of the aortic valve is rare in children. The risk factors for the development of aortic pseudoaneurysms include aortic dissection, infection, arterial wall degeneration, and poor surgical technique. As sudden rupture of an aortic pseudoaneurysm can be fatal, surgical resection of the aneurysm is warranted. In this case, as the pseudoaneurysm was large (18×24×20 mm), the patient underwent surgical pseudoaneurysm resection. We initially discussed whether ascending aortic replacement or Ross operation should be performed; however, as the intraoperative findings showed no sign of aortic valve infection and aortic valve stenosis was not severe, we selected ascending aortic replacement. In our patient, the fragility of the aortic wall due to inflammation from the infective endocarditis could have contributed to the formation of the pseudoaneurysm. Although we could not determine the cause of the aneurysm, infective findings around the aneurysm entry were noted. It was possible that long-term jet flow to the aortic wall from the stenotic aortic valve induced aneurysm formation. Echocardiography revealed that the jet flow was directed towards the right anterior wall of the ascending aorta due to aortic valve stenosis; this was also the entry site of the aneurysm. However, we were unable to prove this hypothesis and regrettably did not check this flow using 4-D flow magnetic resonance imaging. We also could not rule out the effect of the valvoplasty technique.
The most common symptoms of pseudoaneurysms in the ascending aorta are chest pain, heart failure, and sepsis. In contrast, tracheal compression is more commonly associated with pseudoaneurysms in the aortic arch and descending aorta. In our case, the pseudoaneurysm was incidentally detected on echocardiography as the patient did not present any of the common symptoms.
A regular follow-up, including the use of imaging modalities and physical examination, is mandatory to detect such pseudoaneurysms after cardiovascular surgery3). In this case, the unidentified cavity was detected via echocardiography and finally diagnosed as an aortic pseudoaneurysm using contract-enhanced computed tomography. Therefore, we should consider an aortic aneurysm in cases of infective endocarditis of the aortic valve and aortic valve stenosis.
Conflicts of Interest
The authors declare no conflict of interest.
Author Contributions
All other authors have contributed to data collection and interpretation and have critically reviewed the manuscript. All authors approved the final version of the manuscript, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.