Congenital atresia of the left coronary artery ostium closes the origin of the left coronary artery despite the formation of the main trunk of the left coronary artery. Thus, the left coronary blood flow is retrogradely supplied by collateral vessels from the right coronary artery.1) Symptoms include repeated swooning or chest pain during exercise. However, sudden death may also be the first symptom.
We herein report the case of a seven-year-old girl who complained of chest pain on movement with congenital atresia of the left coronary artery ostium. Her myocardial scintigram revealed the rare finding of reverse redistribution phenomenon (reverse redistribution-like findings).
Our female patient was otherwise healthy when encountered, with no history of Kawasaki disease or myocarditis and had no abnormalities in her family history. She was referred to our hospital with a heart murmur when she was two years old. She was diagnosed with moderate mitral regurgitation due to mitral valve prolapse on echocardiography and began taking diuretics. Cardiomegaly improved after starting diuretics. She subsequently presented for outpatient follow-up every three months but never complained of chest pain or shortness of breath. Because of this, we did not suspect coronary artery disease and did not observe the origin of the coronary artery on twice-year echocardiography.
However, at seven years old, she complained of chest pain after climbing a slope on the way to school and was brought to our hospital for an examination.
Her height was 113.9 cm and weight 18.2 kg. No arrhythmia was observed at a heart rate of 75/min. Her blood pressure was 103/79 mmHg, and her respiratory sounds were clear. A Levine II/VI systolic murmur was heard at the apex.
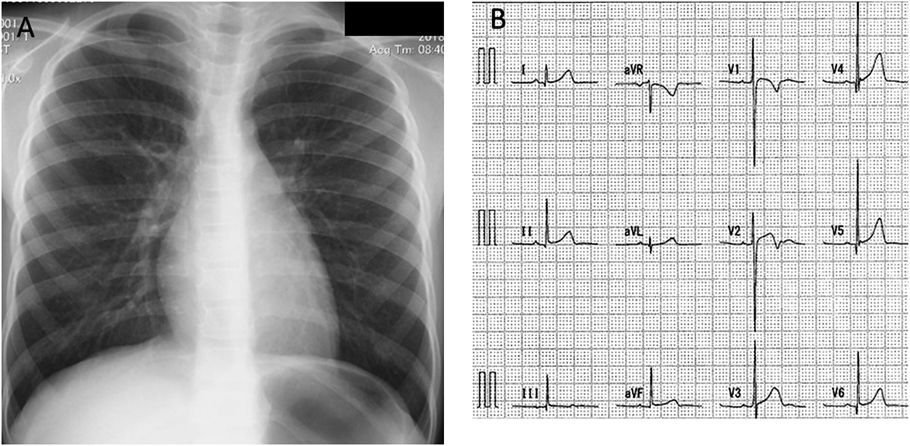
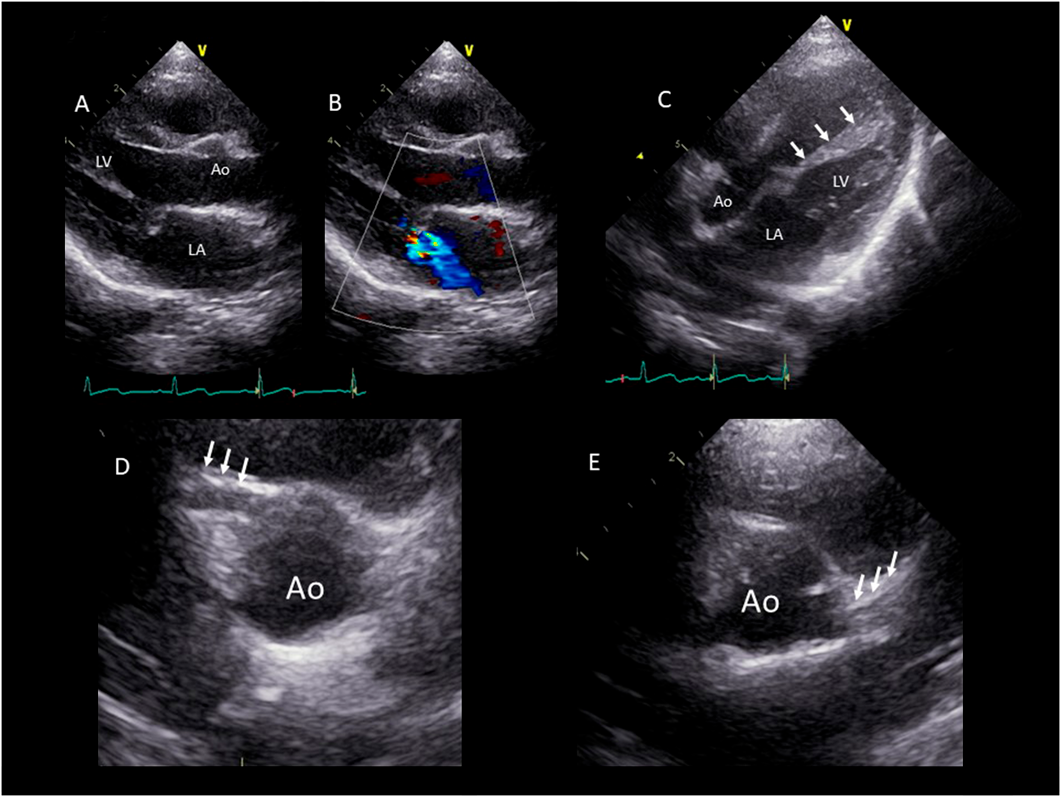
Chest radiograph showed a cardiothoracic ratio of 42%, and a 12-lead electrocardiogram at rest was normal with no ST changes (Fig. 1). Blood tests showed no abnormal findings with a human brain natriuretic peptide (BNP) level of 13.0 pg/mL. Echocardiography findings are shown in Fig. 2. The left ventricular end diastolic diameter was 30.1 mm (84.3% of our normal value), end systole diameter was 19.5 mm with ejection fraction of 70%, and mitral ring annulus diameter 20.9 mm (94.6% of our hospital normal value). The degree of mitral valve regurgitation was moderate according to the Color Doppler method. However, the left atrium/aortic ratio was 1.17, and there was no enlargement of the left atrium.
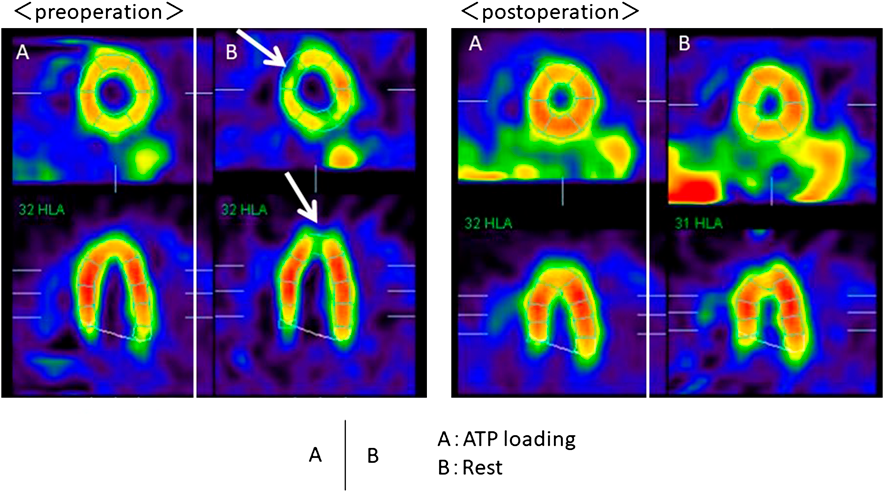
Due to the high echogenicity of the left ventricular papillary muscle, we suspected abnormalities in the left coronary artery. The right coronary artery was enlarged to 3 mm (2.7 in Z-score), whereas the left coronary artery was thin with an unidentifiable origin. Therefore, we performed myocardial scintigraphy using techenetium-99m (99mTc)-tetrofosmin perfusion agents with adenosine loading. Immediately after the adenosine loading, she complained of chest pain with negative conversion of T wave on an electrocardiogram. On adenosine loading, the accumulation of 99mTc-tetrofosmin was slightly decreased from the anterior wall to the apex, but at rest, the accumulation at the same site was further reduced (Fig. 3).
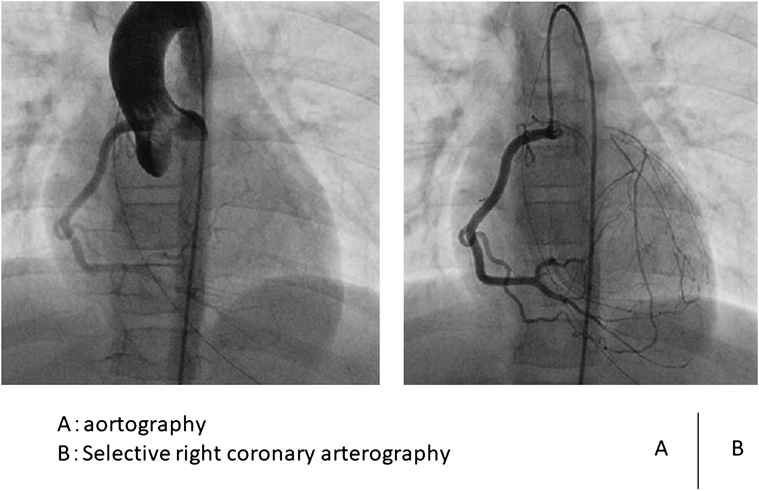
Based on the above findings, we strongly suspected myocardial ischemia. We therefore performed cardiac catheterization and cardiovascular angiography. On left ventricular imaging, the left ventricular end-diastolic volume was 44.4 mL (86% of our normal value), and the ejection fraction was 68.3%. The degree of MR was Sellers II. There was no abnormality in the wall movement. On aortography, the left coronary origin was not detected. On selective right coronary angiography, the left main coronary artery was retrogradely contrasted via collateral circulation (Fig. 4). We diagnosed her with atresia of the left coronary artery ostium based on the results of cardiovascular angiography. Two months later, she underwent bypass surgery with the left internal thoracic artery anastomosed to the left anterior descending coronary artery and mitral valvuloplasty.
After surgery, adenosine-loaded myocardial scintigraphy was performed again. The blood flow had clearly improved from the anterior wall to the apex of the heart (Fig. 3). The chest pain disappeared, so she was able to attend school just like other children.
Various symptoms, such as abnormal ECG findings and chest pain, are important for the diagnosis of coronary artery atresia, but some cases have been detected by autopsy findings. In the present case, the first trigger for consultation was mitral regurgitation. The degree of regurgitation was moderate and required the administration of diuretics. Mitral regurgitation based on myocardial ischemia is believed to be caused by dilation of the left ventricle and mitral valve annulus due to myocardial ischemia. In addition, papillary muscle displacement and mitral valve retention are said to exacerbate functional regurgitation. However, in our case, myocardial scintigraphy showed myocardial ischemia, but angiography showed no enlargement of the left ventricle and mitral valve annulus. On the other hand, the intraoperative findings of the mitral valve revealed a cleft in the posterior leaflet and a papillary muscle elongation in the anterior leaflet. The mitral valve annuloplasty was completed by suturing the cleft and attaching the artificial chords to the extended papillary muscles. Given the above intraoperative findings, the mitral regurgitation in our case was likely related to both the morphological abnormality due to cleft and a functional abnormality of the papillary muscle due to myocardial ischemia. Infant mitral regurgitation is a rare condition, but it is necessary to consider not only morphological abnormalities but also myocardial ischemia.
The onset time of atresia of an orifice of the coronary artery varies from infancy to adulthood.1–5) It is speculated that the onset time depends on the degree of development of the collateral circulation. Thus, a well-developed collateral circulation rendered the present case asymptomatic until seven years old. However, at that point, myocardial ischemia symptoms manifested. Since the amount of exercise increased, the blood flow from the collateral circulation became insufficient, which likely caused the myocardial ischemia.
In the present case, at rest, the decreased accumulation of 99mTc-tetrofosmin was strongly noted on myocardial scintigraphy used 99mTc-tetrofosmin agents with adenosine loading. On cardiac myocardial scintigraphy using thallium, there was no or only a slight decrease in the blood flow at the time of loading.
The phenomenon in which a decrease in the blood flow appears or worsens at rest is called the ‘reverse redistribution phenomenon.’ This phenomenon is observed after coronary revascularization and chronic coronary artery disease. An injured myocardium that has recovered its blood flow has a good initial intake of thallium and can absorb it well. However, myocardium that has been damaged is believed to be unable to retain thallium well, which can lead to the acceleration of washout.6) Because thallium has a long half-life, we can see redistribution and reverse redistribution findings; such findings are not noted with 99mTc-tetrofosmin due to its short half-life.
Regarding why reverse redistribution-like findings were observed on myocardial scintigraphy used 99mTc-tetrofosmin perfusion agents with adenosine loading, several hypotheses have been proposed. Since our patient showed no stenosis in the coronary artery, the coronary artery was able to dilate on adenosine loading, thereby increasing the coronary blood flow and thus the blood flow to the myocardium. The site at which the collateral circulation was well developed therefore accumulated a large amount of 99mTc-tetrofosmin due to the expansion of the collateral circulation. However, since the collateral pathway does not increase or expand at rest, the absorption of 99mTc-tetrofosmin decreases.
Myocardial ischemia in children is difficult to detect. However, if ischemia is suspected, as in present case, active examination may be successful. Myocardial scintigraphy is a relatively minimally invasive and useful examination for myocardial ischemia in children.
Funding
The authors have no funding sources relevant to this article to disclose.
Financial Disclosure
The authors have no financial interests relevant to this article to disclose.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
引用文献References
1) Musiani A, Cernigliaro C, Sansa M, et al: Left main coronary artery atresia: Literature review and therapeutical considerations. Eur J Cardiothorac Surg 1997; 11: 505–514
2) Gerlis LM, Magee AG, Sheppard MN: Congenital atresia of the orifice of the left coronary artery. Cardiol Young 2002; 12: 57–62
3) Van der Hauwaert LG, Dumoulin M, Moerman P: Congenital atresia of left coronary ostium. Br Heart J 1982; 48: 298–300
4) Leivo IV, Laulia PK: Atresia of left coronary ostium and left main coronary artery. Arch Pathol Lab Med 1987; 111: 1173–1175
5) Sohn SY, Jang GY, Choi BM: Congenital atresia of left main coronary artery in an infant. J Zhejiang Univ Sci B 2010; 11: 539–541
6) Hashimoto J, Suzuki T, Nakahara T, et al: Preoperative risk stratification using stress myocardial perfusion scintigraphy with electrocardiographic gating. J Nucl Med 2003; 44: 385–390