Cor triatriatum dexter (CTD) is an extremely rare congenital cardiac malformation in which a persistent embryonic right sinus venosus valve subdivides the right atrium (RA).
Septation of the RA can interfere with normal blood flow into the RA and tricuspid valve, leading to a broad range of clinical symptoms. Depending on the degree of RA obstruction, a clinical sign of these anatomic variations may be neonatal cyanosis necessitating urgent surgical intervention while some patients are asymptomatic and reach adulthood without therapy.1)
To our knowledge, there have not been any reports of infants with a hypoplastic RV who were diagnosed with CTD, and there is no consistent opinion about the best treatment strategy for this condition. In this case report, we describe a male neonate with CTD and a hypoplastic RV who had symptoms of central cyanosis soon after birth. In this patient, a large membranous structure was identified in the RA and flow from the IVC was partially redirected into the LA via the patent foramen ovale (PFO).
The guardians of the patient, whose details appear in this report, provided verbal informed consent, and the study’s design was approved by the appropriate ethics review board.
A male neonate was spontaneously born at 40 weeks of gestation after an uncomplicated pregnancy, and his birth weight was 3,310 g. His Apgar score was 9 and 10 at 1 and 5 min, respectively. At 3 hours after birth, his physical examination revealed the presence of central cyanosis with a room air oxygen saturation value between 85% and 93%. The patient was unresponsive to oxygen administration, and the room air oxygen saturation level decreased to below low 70% with crying. The patient was otherwise well, with no signs of respiratory distress.
Transthoracic echocardiography was performed at an outside hospital and showed tricuspid valve stenosis and closing ductus arteriosus. A prostaglandin E1 infusion was started and the neonate was transferred to our institution. Upon admission, his saturation values remained around 85%–90%, although he had patency and an adequate ductal size. His vital signs, except for oxygen desaturation, were within normal range. His cardiovascular examination showed a quiet precordium, normal heart sounds, and no murmur. The results of all investigations including complete blood count, septic work-up, and liver and renal function tests were normal, but only the plasma brain natriuretic peptide level was elevated to 131 pg/mL. The venous blood gas pH was 7.45 and the PaCO2 was 35.8 mmHg, and the base excess was +1.7 mmol/l. The findings of chest radiography and electrocardiography were also unremarkable.
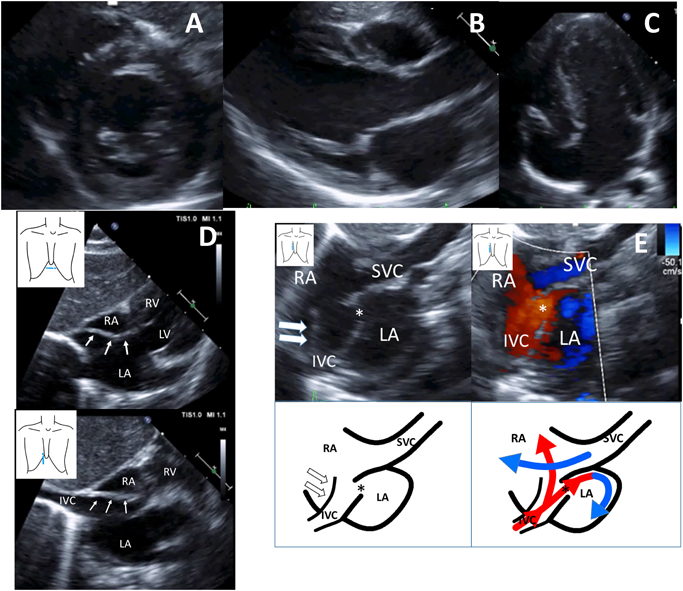
Using two-dimensional transthoracic echocardiography, we diagnosed the neonate with congenital tricuspid valve stenosis with a hypoplastic RV at first (Fig. 1A–C) and continued administering prostaglandin E1 infusion. The tricuspid valve was hypoplastic and dysplastic with trivial tricuspid regurgitation (the annulus measured 6.0 mm; the normal range is 9.3–17.5 mm; z-value, −3.9). The inflow of the tricuspid valve appeared to be substantially narrowed with an eccentric jet crossing from the RA to the hypoplastic RV. A pulse-wave Doppler ultrasound examination of the tricuspid valve’s inflow revealed it had a monophasic pattern with maximal velocities of 1.4 m/s. The pulmonary valve’s annulus was smaller (6.6 mm; the normal range is 5.9–9.8 mm; Z-value −0.93), but there was no evidence of abnormal valve thickening or flow acceleration and valve regurgitation on color or pulsed Doppler ultrasound examinations.
A few days later, we noticed there was a prominent and elongated membranous structure extending from the junction of the IVC to the RA (Fig. 1D). Color Doppler ultrasound with a right sternal border sagittal view showed that the large membranous structure hemodynamically divided the RA into two chambers; that is, both blood flow from the IVC and superior vena cava (SVC) were partially redirected by this membrane to the LA via the PFO, leading us to diagnose the patient with CTD (Fig. 1E). After stopping prostaglandin E1 infusion, we confirmed that the ductus arteriosus was closed, and the patient’s saturation values remained at approximately 85%–93% with oxygen inhalation (1 L/min nasal cannula).
Upon serial evaluation with transthoracic echocardiography, we found that the tricuspid and pulmonary valve diameters gradually grew in the postnatal period (Table 1). We judged that elective surgery was possible, and the patient was sent home with standby oxygen and a pulse oximeter at 33 days after birth.
Table 1 Serial measurements of echocardiographic parameters and SpO2| Measurement parameters | Day0 | Day12 | Day20 | Day27 | Day48 | 2months old | 3months old |
|---|
| Tricuspid valve diameter (mm) | 6.0 | 6.3 | 6.1 | 7.0 | 7.3 | 9.3 | 9.8 |
| Z-value | −3.9 | | | | −3.8 | | −2.8 |
| Pulmonary valve diameter (mm) | 6.6 | 5.7 | 6.3 | 7.4 | 7.0 | | 7.2 |
| Main pulmonary artery diameter (mm) | 7.0 | | 5.8 | 6.9 | 7.0 | | 7.4 |
| TVd/MVd | | 0.49 | 0.51 | 0.54 | | 0.61 | 0.61 |
| TVd: tricuspid valve diameter | | | | | | | |
| MVd: mitral valve diameter | | | | | | | |
| est Qp (L/min/m2) by VTI | | 2.4 | 2.3 | 2.6 | 2.3 | | 2.4 |
| est Qp/Qs by VTI | | | 0.61 | 0.60 | | | 0.85 |
| SpO2 (%) room air | 87–93% | | | | | 77–88% | 75–86% |
| SpO2 (%) O2 inhalation | | 84–91 | 85–93 | 87–93 | 88–92 | 87–92 | 85–90 |
| Body weight (g) | 3,310 | | | 4,600 | 5,988 | | 8,695 |
| Qp, pulmonary blood flow; Qs, systemic blood flow; RV, right ventricle; VTI, velocity time integral |
Since desaturation progressed, we performed cardiac catheterization when the patient was 3 months old. Angiography of the SVC showed that contrast media mainly flowed toward the tricuspid valve into the RV (Fig. 2A). Similar to the echocardiographic findings, the tricuspid valve’s diameter and RV volume were small (Fig. 2B, C). We performed a balloon occlusion test of the foramen ovale (FO) and compared the hemodynamic parameters and angiographic findings before and after the balloon occlusion test (Table 2). Considering the end-diastolic volume of the RV (RVEDV) and tricuspid valve’s diameter, we judged that partial closure of the FO was more preferable than total closure.
Table 2 Cardiac catheterization data| (A) ‹Preoperative data› room air |
|---|
| Pre balloon occlusion | Post balloon occlusion |
|---|
| RAP | 8/6/(6) | 8/7/(7) |
| RVP | 20/EDP 5 | 14/EDP 7 |
| MPAP | 19/10/(14) | 19/10/(14) |
| SaO2(DAO) | 90 | 95 |
| Qs (Fick) | 4.2 | 4.1 |
| Qp/Qs | 0.74 | — |
| Rp(U・m2) | 1.2 | 1.3 |
| RVEDV(mL) | 9.2 (50%N) | 9.7 (53%N) |
| RVEF(%) | 54 | 49 |
| PA index | 179 | — |
| (B) ‹Postoperative data› room air |
|---|
| RAP | 6/6/(4) | |
| RVP | 19/EDP 5 | |
| MPAP | 17/3/(9) | |
| SaO2(DAO) | 97 | |
| Qp/Qs | 0.9 | |
| Rp(U・m2) | 0.5 | |
| RVEDV(mL) | 21.4 (78%N) | |
| RVEF(%) | 54 | |
| PA index | 258 | |
| DAO, discending aorta; EDP, end diastolic pressure; MPAP, main pulmonary arterial pressure; PA index, pulmonary arterial index; Qp, pulmonary blood flow; Qs, systemic blood flow; RAP, right atrial pressure; Rp, pulmonary resistance; RVEDV, right ventricular end-diastolic volume; RVEF, right ventricular ejection fraction; RVP, right ventricular pressure; SaO2, arterial oxygen saturation O2 |
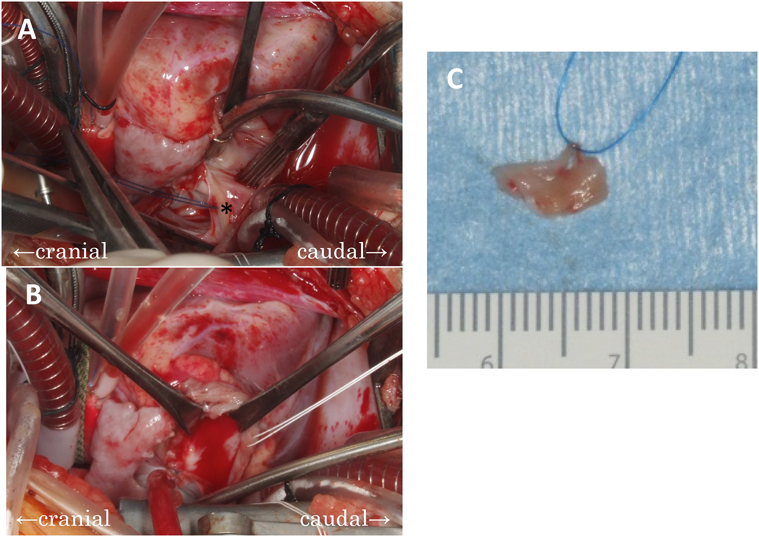
We performed surgery (resection of the large persistent right sinus venosus valve and partial closure of the PFO) when the patient was 4 months old and had a body weight of 9.1 kg. We performed cardiopulmonary bypass with cardioplegic arrest. The large membrane that originated from the crista terminalis and Eustachian valve covered half of the caudalis of the FO, and we completely resected it by separating its attachment (Fig. 3). The tricuspid valve’s diameter was 11 mm (61% of the normal diameter) and had a dysplastic appearance, and the PFO was approximately 6 mm. We finally decided to close the FO partially, and we sewed only the right border of the FO and reefed it to 4 mm.
The neonate’s postoperative course was uneventful. An echocardiogram showed that he had normal cardiac function, the large membranous structure in the RA had disappeared, and flow from the IVC was mainly directed into the tricuspid valve with a small right-to-left shunt through the partially closed FO. The patient was transferred to the general ward of our hospital on the second day postoperatively and was discharged on the 12th postoperative day. After surgery, his room air saturation level remained around 90%, and it increased to 95%–97% with the administration of oxygen, so he was sent home with standby oxygen.
The patient’s room air saturation values increased and remained around 94% beginning 3 months after surgery and remained at around 95%–96% beginning 6 months after surgery; therefore, we administered home oxygen therapy 7 months after surgery (Table 3). We performed cardiac catheterization 12 months after surgery and confirmed that the RV was well-developed and had good function (Fig. 2D, E). We expected that the PFO would close spontaneously during the follow-up period.
Table 3 Serial post-operative measurements of echocardiographic parameters and SpO2| Measurement parameters | Preoperation | Postoperation |
|---|
| 9 days | 1 month | 2 months | 3 months | 6 months | 12 months |
|---|
| Tricuspid valve diameter (mm) | 9.8 | 10 | 8.5 | 10.6 | | 10.3 | 13.1 |
| Z-value | | | | Z=−2.3 | | | Z=−2.0 |
| Pulmonary valve diameter (mm) | 7.3 | 10.3 | | | | | 12.0 |
| TVd/MVd | | | | 0.58 | | | 0.66 |
| TVd: tricuspid valve diameter | | | | | | | |
| MVd: mitral valve diameter | | | | | | | |
| RV inflow (cm/s) | | E<A | | E82<A105 | E<A | E>A | E101>A93 |
| Qp (L/min/m2) by VTI | 2.4 | 2.7 | | 3.0 | | | |
| SpO2 (%) room air | 88 | 91–92 | 91–92 | 90–91 | 94 | 95–96 | 99 |
| SpO2 (%) O2 inhalation | 93 | 95 | 96 | 94–97 | 94–95 | 96 | |
| O2 flow rate (L/min) | 1 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 off | |
| Qp, pulmonary blood flow; Qs, systemic blood flow; RV, right ventricle; VTI, velocity time integral |
In this case report, we described a male neonate with CTD with a hypoplastic RV who had symptoms of central cyanosis soon after birth. A large membranous structure was identified in the RA and flow from the IVC was partially redirected into the LA via the PFO. We surgically resected the large membranous structure and partially closed the FO when the patient was 4 months old and the patient had a good clinical course.
During the embryonic development of the heart, the right horn of the sinus venosus is incorporated into the RA, giving rise to the orifices of the SVC and IVC. At one point, the right valve of the sinus venosus nearly divided the RA. It is considered to be a functional valve in the fetus that helps direct oxygenated blood from the IVC toward the FO, thereby bypassing pulmonary circulation.2) With the growth of the heart, early in the fetal (between 9 and 15 weeks of gestation), the valve regresses and moves caudally, leaving the crista terminalis as its cephalic remnant in a mature heart and the valves of the IVC (Eustachian valve) and coronary sinus (Thebesian valve) as its caudal remnants. A minor degree of RA septation is well tolerated, and a prominent Eustachian valve is a common finding on two-dimensional echocardiography. However, a large, sail-like membrane that fails to regress may obstruct the tricuspid valve, RV outflow tract, or IVC and affect the patient’s hemodynamics. It has been hypothesized that failed regression of the venous valve may lead to fetal circulatory abnormalities and subsequent underdevelopment of the right heart’s structures in utero.3)
The clinical presentation of patients with CTD is slightly variable. Most patients are asymptomatic, and a lesion is discovered during echocardiography or surgery to correct other cardiac lesions. Cyanosis may occur in those with associated interatrial communication due to a large right-to-left shunt when flow from the IVC is redirected into the LA via interatrial communication. Our patient had cyanosis soon after birth. We believe that the membranous structure in the RA was large enough, and anterior deviation of the atrial secundum septum permitted blood flow to be redirected from the IVC into LA. This right-to-left shunt across the PFO explains why basal desaturation was unresponsive to oxygen. The left valve of the sinus venosus retrogressed and was absorbed into the limbus region of the septum secundum. It is thought that abnormal development and absorption of the left valve of the sinus venous are related to anterior deviation of the septum secundum.
When accompanied with interatrial communication, a right-to-left shunt may be observed, and the patient may be misdiagnosed with a tricuspid valve anomaly. In our case, we misdiagnosed the patient as having congenital tricuspid stenosis at first. Congenital tricuspid stenosis is usually associated with other anomalies, especially RV tract obstruction or atresia with secondary hypoplasia of the RV.
Clinically, tricuspid valvular stenosis can be distinguished from hypoplasia of the tricuspid valve. In patients with tricuspid valvar stenosis, the tricuspid annulus may be relatively large, but its leaflets are thickened with commissural fusion and shortened chordae tendineae. In those with hypoplasia of the tricuspid valve, the tricuspid valve’s annulus is small, and its leaflets and chordae may be diminutive but otherwise normal. Our patient had a small tricuspid valve diameter; thus, we should have diagnosed him with hypoplasia of the tricuspid valve rather than congenital tricuspid valve stenosis, but the RV outflow tract was intact. In a patient with a small tricuspid valve diameter and without RV outflow tract obstruction or atresia, it is important to detect the RA by considering the possibility of a persistent right sinus venosus valve.
Intervention is indicated for patients who are symptomatic. Recently, disruption of the obstructing membrane with a percutaneous catheter has been reported,4) and this may be the therapy of choice in adult patients. In pediatric patients, there are no similar reports, and surgical correction is prevalent when intervention is necessary. Surgical resection is warranted when the symptoms of flow obstruction or persistent desaturation are observed.5) In previous reports, the timing of intervention was different between newborns and adults.6, 7) Some previous reports showed that some neonates present with cyanosis during the newborn period, but improved naturally afterwards; therefore, waiting for natural growth is one of the treatment strategies.8)
In this case, we observed the neonate for 3 months considering the following points: permissible range of hypoxemia on oxygen supply; serial development of tricuspid valve diameter; and the possibility of spontaneous regression of Eustachian valve. We initially wanted to observe the patient’s natural improvement, but natural improvement was not observed. Due to progressive desaturation, small RV volume by angiography, and necessity for resection of the Eustachian valve and also intervention for the PFO, we deemed surgical intervention to be necessary. In our case, whether we could totally close the FO or not was an important clinical point because of the small RV volume. As there are no reports similar to our case, we extrapolated the RV-TV (tricuspid valve) index used in the operative method selection criteria for pulmonary atresia with intact ventricular septum.
The RV-TV index was 0.29 in our case (RVEDV 50%N, tricuspid valve diameter: 58% of normal), and we believe that this indicated partial closure of the FO (4-mm fenestration). As a result, cyanosis remained after the surgical operation, but it gradually improved as the right ventricle grew.
If we had performed total closure of the FO, we believe that the patient would have been more likely to suffer from right heart failure, although there was a possibility of earlier right ventricular development.
We speculate that for CTD with hypoplastic RV and inter-atrial communication, resection of the Eustachian valve, and partial closure of the FO may be effective treatment strategies as long as the size of the RV is taken into consideration. Further studies on the RV size and intervention for the FO in such cases of CTD are needed.
謝辞Acknowledgments
We would like to thank Editage (www.editage.jp) for English-language editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
引用文献References
1) Chad A, Jennifer L, Ronald K, et al: A case series of patients with cor triatriatum dexter: Unique cause of neonatal cyanosis. Pediatr Cardiol 2015; 36: 240–243
2) Condoluci C, di Donato RM, Marcelletti C, et al: Central cyanosis in a newborn infant due to a prominence of the eustachian valve. G Ital Cardiol 1994; 24: 151–154 (in Italian)
3) Schutte DA, Rowland DG, Allen HD, et al: Prominent venous valves in hypoplastic right hearts. Am Heart J 1997; 134: 527–531
4) Savas V, Samyn J, Schreiber TL, et al: Cor triatriatum dexter: Recognition and percutaneous transluminal correction. Cathet Cardiovasc Diagn 1991; 23: 183–186
5) Carton AJ, Rocafort AG, Rubio D, et al: Persistent embryonic right venous valve giving a cor triatriatum dexter appearance in a cyanotic neonate. J Thorac Cardiovasc Surg 2011; 142: e147–e148
6) Tueche S: Cor triatriatum dextrum. Surgical treatment in a neonate. Acta Cardiol 2003; 58: 39–40
7) Vukovic PM, Kosevic D, Milicic M, et al: Cor triatriatum dexter and atrial septal defect in a 43-year-old woman. Tex Heart Inst J 2014; 41: 418–420
8) Waragai O, Boku H: A case of cortriatriatum dexter. Nihon Syuusanki Sinseiji Igakukaisi 2005; 41: 372 (in Japanese)