Recognition of Preclinical Cardiomyopathies
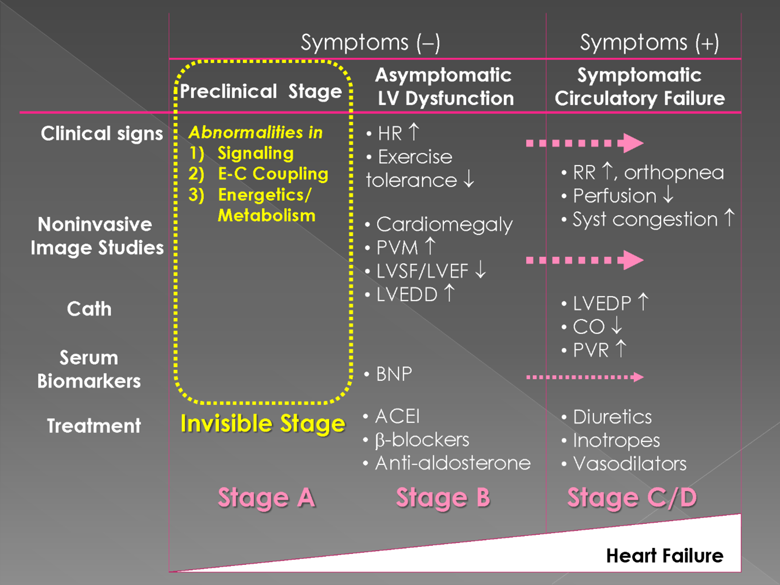
A classification of chronic HF in adults was published in 2005 by the American Heart Association (AHA)/American College of Cardiology (ACC)2) (Table 1). In this classification, Stage A was defined as a “preclinical” stage, where certain functional deterioration at the cellular level is present but is not enough to cause “visible” morphological changes, including ventricular dysfunction or dilatation. This stage inevitably progresses to Stage B, where tissue- or organ-level abnormality is commonly detected as ventricular dysfunction or dilatation by non-invasive imaging studies but without HF symptoms. Symptoms of HF arise once the low cardiac output persists and/or ventricular filling is compromised to induce venous congestion (Stage C) (Fig. 1). Multiple organs, including kidney, lung, liver, brain, bone, and skeletal muscles, are involved in worsening of clinically overt HF, suggesting that the advanced HF (Stage D) is a disease of multiple organ failure as a consequence of disrupted inter-organ biological crosstalk.3, 4)
Table 1 ACC/AHA 2005 Guideline Update for Diagnosis and Management of Chronic Heart Failure in Adults2)| Stage A | At high risk of HF† |
| Structural heart disease§ (−). Symptoms (−) |
| Stage B | Structural heart disease§ (+). Symptoms (−) |
| Stage C | Structural heart disease§ (+). Symptoms (+) |
| Stage D | Refractory CHF requiring specialized interventions |
| † Patients with hypertension, atherosclerosis, diabetes, obesity, or metabolic syndrome or using cardiotoxins or FH of CM. § Ventricular dilatation or hypertrophy. |
In the field of pediatrics, we encounter two relatively common patient populations with preclinical HF that are programmed to develop overt HF in a chronic phase. These include Duchenne muscular dystrophy (DMD) and anthracycline-induced cardiotoxicity (AIC). These two disorders recently have gained immense scientific interest because they serve as an excellent human model to understand the evolution of HF from preclinical to advanced stages with the availability of experimental animal models.5–8) The development of cardiomyopathy and clinical symptoms of HF is insidious but may progress to reach medically refractory HF (Stage D) in late teens in DMD9, 10) and early to mid-adulthood in AIC.11–13)
Duchenne muscular dystrophy is an X-linked genetic disorder that causes progressive weakness and wasting of skeletal muscle and myocardium in boys affecting one in 3,600 to 9,300 live male birth due to mutation of dystrophin.14, 15) The structural integrity of each individual skeletal and cardiac myocyte is significantly compromised upon physical stress due to absence of dytrophin,16–18) but the underlying mechanisms of muscle wasting are more complex, involving multiple different processes, including intracellular calcium overload,19–22) alteration in the nitric oxide (NO) pathway,23, 24) increased reactive oxygen species (ROS) and mitochondrial dysfunction,25–27) and extracellular matrix remodeling and myocardial fibrosis.28–31) There are certain other factors involved in the pathogenesis of DMD cardiomyopathy, including epigenetic factors, post-translational modification, telomere dysfunction, and genetic modifiers.32, 33) Dystrophin deficiency perturbs physiological myocyte growth in response to increased biomechanical stress as dystrophin serves as a mechanosensor that regulates protein synthesis via the NO pathway.24) Pathological alteration of DMD myocardium is heterogeneous34) and probably a combined consequence of myocardial wasting (myocyte loss or atrophy)35, 36) and secondary geometric changes (remodeling).37) The chamber dilatation and ventricular wall thinning occur in combination with secondary fatty infiltration and fibrosis upon myocyte death.38, 39) The earliest signs of cardiomyopathy in asymptomatic DMD are either decreased systolic function40) or resting sinus tachycardia.41) The mechanism of resting tachycardia is not well understood, but it is thought to be secondary to dysautonomia42) and/or decreased myocardial compliance due to fibrosis.41) The early clinical manifestation of HF is frequently overlooked, as most DMD patients usually become non-ambulatory and reliant on a wheelchair by age 13 because of progressive muscle weakness and wasting.37) Recent guidelines by American Heart Association suggested early prophylactic treatment with Angiotensin II-converting enzyme inhibitor (ACEi) before age 10 years regardless of left ventricular (LV) function.43)
Survivors of childhood cancer who received anthracycline therapy have a life-long risk of developing HF.11, 44–48) Several risk factors are known to affect the clinical course, including the cumulative dose of anthracycline, female sex, younger age at treatment, radiation therapy, genetic predisposition, and traditional risk factors for adult heart disease (hypertension, diabetes, smoking, hyperlipidemia, and obesity).49–51) The underlying mechanism of AIC is poorly understood but is thought to be multifactorial with complex mutual interactions,52–56) including increased ROS production,57, 58) intracellular calcium overload,59, 60) disrupted sarcolemmal integrity,61) mitochondrial dysfunction due to iron overload62) or enhanced autophagy,8) damaged DNA replication by topoisomerase 2β,63) impairment of cell survival pathways (neuregulin/ErbB signaling),64) premature senescence,65–67) and damage of cardiac stem cells.7, 66) These process are responsible for cardiomyocyte death and permanent myocardial injury through a common pathway of calcium overload, lipid peroxidation, and mitochondrial dysfunction,68) resulting in ventricular wall thinning, increased wall stress, ventricular dysfunction, and, eventually, DCM. Inadequate ventricular mass with chronic afterload excess may explain the persistent and progressive nature of AIC.12) One big mystery is the temporal gap between initial anthracycline exposure and initiation of cardiovascular adverse effects.52)
Based upon the onset, AIC is classified as a) acute (during or within 1 week of treatment: incidence <1%), b) early chronic (<1 year after treatment: ∼2%), and c) late-onset chronic (>1 year or a few decades after treatment: 5 to 57%).44, 51) Acute cardiotoxicity is relatively reversible, whereas late-onset chronic type is slowly progressive and irreversible that commonly leads to medically refractory HF. The incidence of cardiomyopathy in children who have received anthracycline-based chemotherapy is estimated at 3.3% at 10 years and 4.8% at 15 years,69) but the incidence of adverse cardiovascular events is higher with longer follow-up periods.48, 51, 70) The majority of the affected children remain asymptomatic with normal ventricular function during childhood, but the pathological process might have already been initiated at the molecular and cellular levels. As most of the late onset chronic cardiotoxicity presents during early to middle adulthood, it rarely catches the attention of pediatric medical providers unless there is an identifiable LV dysfunction. It is clear that detection of this preclinical phase gives us the best opportunity to impact the progression to the irreversible and life-threatening end-stage disease, at which point medical treatment has limited efficacy. The recommendations for primary surveillance to detect occult cardiotoxicity were published by Armenian and colleagues, optimizing the opportunities for collaborative research.71)
The underlying pathobiology of cardiomyopathy in DCM and AIC is summarized in Fig. 2. There are similarities between the two as myocyte death and subsequent wall thinning comprise a primary pathogenesis of both cardiomyopathies. In DMD cardiomyopathy, dysautonomia frequently causes persistent tachycardia, which increases myocardial oxygen demand. Because progressive myocyte loss and deficient LV mass predominates in DMD cardiomyopathy, ventricular dilatation may not be always evident even in the advanced stage. On the other hand, in AIC, cytotoxic effects target not only cardiomyocytes but also non-myocytes including endothelial cells, cardiac fibroblasts, and cardiac progenitor cells.11) Cardioprotective vascular development in response to ischemic injury and/or increased biomechanical stress may be mitigated, in part, due to disruption of paracrine crosstalk between the cells that plays a protective role against the adverse remodeling, responsible for an early onset of ischemic heart disease.64)
Diagnosis of Preclinical HF in Children
Echocardiography
Detecting subtle ventricular dysfunction and subclinical HF is a diagnostic challenge. Left ventricular systolic function can be assessed with measurement of shortening fraction (SF) on two-dimensional (2D) or M-mode short axis parasternal images. Shortening fraction simply reflects a change in LV chamber dimension during the cardiac cycle.
The Children’s Oncology Group adopted SF as a way of assessing the effect of chemotherapy on the heart. Shortening fraction is, however, limited in several ways: 1) it is obtained in one view and does not reflect motion of all of the cardiac segments; 2) it is unreliable in the setting of regional wall motion abnormalities, most notably changes in septal motion, which are common; and 3) it is affected both by preload and afterload.72, 73)
Ejection fraction (EF) has played a central role in the assessment of LV function in numerous adult clinical trials. Initial EF measurements were performed using gated radionuclide scans. Low EF measured with this technology was shown to correlate with increased mortality following myocardial infarction.74) Ejection fraction describes the change in volume during the cardiac cycle and is calculated as follows:
The numerator measures stroke volume (SV), which varies directly with EF. The denominator assesses the degree of dilation, which varies inversely with EF. Several formulas have been developed, taking into account the ellipsoid shape of the LV and using the linear chamber diameter, as measured for SF, to then calculate an estimate of EF.72, 73) One of the more commonly utilized approaches is the Teichholz method, which uses this equation: Volume is measured with this formula at end-diastole and end-systole, allowing calculation of SV and EF.
Currently, the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) recommend using the biplane Simpson’s method of multiple discs to calculate LV volumes and EF in adults.75) To accomplish this calculation, the LV endocardial border is traced in two orthogonal planes (typically apical four-chamber and apical two-chamber views or the equivalent transesophageal echocardiographic [TEE] views) at end-diastole and end-systole. A computer algorithm then divides the traced area into 20 discs of equal height and sums the volume of each disc. The endocardial tracing is performed automatically on most current generation echocardiography machines. Manual adjustment of the borders remains important to consistently exclude trabeculations, exclude noise in the near field (apex), and assess for fairly uniform wall thickness. The biplane Simpson’s EF does correlate with outcomes and mortality in adults.76) Limitations include poor endocardial definition due to limited acoustic windows, diminished reliability in the setting of arrhythmia and difficulty defining end-systole and end-diastole when there is significant dyssynchrony.73)
In pediatric patients, SF and EF have been shown to be associated with prognosis in DCM. In a study of 1,426 children with DCM undertaken between 1996 and 2003, independent risk factors for subsequent death or transplantation included older age, congestive HF, cause of DCM, and lower LVSF z score (p<0.001 for all).77) A meta-analysis of pediatric DCM by Alvarez et al. indicated that higher LV EF and SF at diagnosis were predictive of better prognosis across multiple articles. Younger age at diagnosis and the presence of myocarditis as the etiology were also associated with better prognosis.78) The outcomes of 1953 children with DCM over two decades by the Pediatric Cardiomyopathy Registry demonstrated that worse LV SF at diagnosis independently predicted death.79) Echocardiographic parameters of LVSF z score and LVEDD z score predicted a higher risk of sudden death in 289 children with DCM, HCM, LV noncompaction cardiomyopathy, and arrhythmogenic cardiomyopathy.80) While these measures are very useful in overt HF, they are not sufficiently sensitive to detect preclinical myocardial dysfunction. This is particularly true in pediatric patients given the challenges with reproducibility.
Assessment of diastolic function is important but challenging, particularly in children.81) Diastolic dysfunction typically accompanies overt systolic dysfunction but can occur independently in the setting of hypertrophic cardiomyopathy (HCM), restrictive cardiomyopathy (RCM), or in patients with HF preserved EF (HFpEF).82) Changes in diastolic function can also precede systolic dysfunction. Echocardiography is an important means of assessing diastolic dysfunction and utilizes the following parameters:
- 1) Transmitral Doppler inflow pattern: Early filling (E wave) and late filling (A wave) velocities are measured in an apical four chamber view, and E/A ratio is calculated. Moving to an apical five-chamber view and placing the sample volume midway between the mitral leaflet tips and the LV outflow tract, isovolumic relaxation time (IVRT), acceleration time (AT), and deceleration time (DT) are measured from the Doppler tracing.
- 2) Pulmonary venous Doppler flow pattern: The flow pattern at the right upper pulmonary vein is characterized by an initial S wave during systole, a D wave during diastole and an A wave, representing reversal of flow from the left atrium into the pulmonary veins during atrial systole.
- 3) Tissue Doppler imaging (TDI): TDI assesses myocardial motion rather than blood flow. The sample volume is placed within the myocardial tissue immediately adjacent to the septal and lateral hinge-points of the mitral valve. Early (E′) and late (A′) velocities can be measured. A ratio of the mitral inflow E velocity to the tissue Doppler E′ velocity is typically calculated (E/E′ ratio).
- 4) Color M-mode flow propagation velocity (Vp): This measurement is obtained by placing the M-mode cursor through the center of the mitral inflow jet in an apical four-chamber view. The velocity of propagation is the slope of the first aliasing velocity during early filling or the slope of the line where there is a transition from no color to color.
In children, the adult guidelines for assessment of diastolic function do not perform as well. In a 2013 study, three highly-respected investigators, Dragulescu, Mertens, and Friedberg, each measured parameters of diastolic function in 175 children, including patients with DCM, HCM, RCM and a control group. Despite elevated filling pressures in half of the patients, echocardiographic parameters were abnormal in only 14% of the HCM group and in none of the DCM and RCM groups. There was poor interobserver agreement on grading of the diastolic dysfunction using the adult algorithm. Using pediatric reference data rather than the adult data yielded slightly better results, classifying all of the controls as normal, but diastolic dysfunction was detected in only a small proportion of the patients despite severe disease.83)
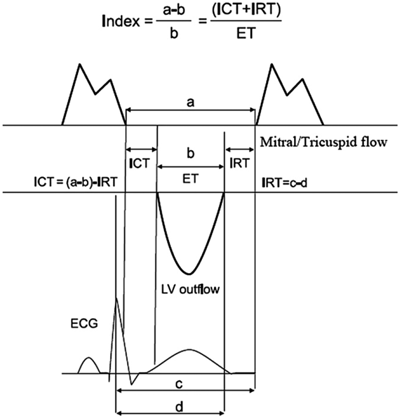
The myocardial performance index (MPI), or Tei index, assesses global ventricular function.84) It is obtained by dividing the sum of the isovolumic contraction time (ICT) plus isovolumic relaxation time (IVRT) by the ejection time (ET). In practice, it is easier to measure the interval from cessation to onset of mitral inflow (a) minus the ET (b) as a substitute for ICT+IRT (Fig. 3). The MPI can be measured on the mitral or tricuspid inflow Doppler or can be measured on tissue Doppler tracings. Compared with Doppler-derived MPI, TDI-derived measurements have the advantage of being less affected by loading conditions and heart rate and more sensitive to diastolic function. In one small study of 25 pediatric patients with HF, TDI-derived septal MPI was inversely correlated with SF and reflected severity of disease. As with SF and EF, MPI is most useful in patients with overt HF and less useful in detection of early or subclinical ventricular myocardial changes. A prospective study in 2010 compared the E/E′ ratio and MPI to near-simultaneous catheter derived hemodynamic parameters in post-transplant children. The correlations were poor.85)
A breakthrough in the ability to assess subtle ventricular dysfunction came with the development of strain echocardiography.86, 87) Strain is based on speckle-tracking technology, which follows a point on the myocardium as it moves through the cardiac cycle. This technology highlights the complexity of myocardial deformation; the ventricle shortens, thickens and twists during systole to eject blood. This angle-independent technique allows quantification of segmental and global ventricular function. Strain can be measured in longitudinal, circumferential and radial planes. The vast majority of data thus far are focused on global longitudinal strain (GLS), which is measured in apical four-chamber, three-chamber, and two-chamber views. Normal values for GLS range from −19% to −20%. In the adult literature, GLS is a valuable prognostic tool and an independent predictor of all-cause mortality in HF patients.88) In multiple studies of adult patients who have undergone chemotherapy, changes in GLS consistently precede significant changes in EF89) and predict cardiotoxicity.90) In a longitudinal study of 737 adult patients, lower (less negative) baseline GLS values predicted mortality in asymptomatic patients with primary mitral regurgitation and preserved EF.91)
Cardiac MRI
Cardiac MRI (CMRI) is currently the reference standard imaging modality for the quantification of ventricular volumes, mass, and EF.92, 93) It has high temporal and spatial resolution in the assessment of RV and LV volume, systolic function, and mass with high interobserver and intraobserver reproducibility.94–96) In contrast to echocardiography, CMRI can obtain high-resolution cine images of the heart in any imaging plane without the limitations of acoustic windows. Normal values are now available on RV and LV volume, mass, and EF for different age groups in males and females, including children.97) Steady-state free precession (SSFP) cine imaging is the current standard method for measuring volumetry in CMRI, replacing cine gradient echo sequences. Cardiac MRI is increasingly used for evaluation, management, and prognosis of patients with HF.92, 93) The method of discs is used for quantification of RV and LV end diastolic and end systolic volumes, and EF can be calculated without making geometric assumptions; this makes CMRI suitable even with dilated and remodeled ventricles.98) In adult patients with HF, EF is a well-recognized factor in the long-term prognosis and survival.99) In the pediatric population, limited data have shown that indices of LV systolic performance such as EF and SF are major determinants of prognosis, in addition to age, presence of congestive HF, and LV dimension z score.100)
Late gadolinium enhancement (LGE) is an MRI sequence that uses gadolinium (Gd) contrast to evaluate for fibrosis in the ventricular myocardium. Gadolinium distributes into the extracellular space of the myocardium but not into the normal myocardial cells.101, 102) In areas of myocardial cell necrosis, there is an increase in Gd distribution into the cells with loss of cell membrane integrity and into the expanded extracellular matrix.103) The increased Gd results in shortened T1 values of the affected areas that results in increased signal intensity on special T1-weighted MRI sequences, such as inversion recovery gradient echo images.104) In adult patients with nonischemic DCM, Assomull et al. showed that midwall fibrosis was present in about 35% of patients and was a predictor of death or hospitalization for cardiovascular events (hazard ratio 3.4) in addition to sudden cardiac death and ventricular tachycardia (hazard ratio 5.2), independent of other factors such as EF.105)
More recent and newer CMRI techniques have emerged to quantify fibrosis in cardiomyopathies in addition to providing a more accurate volume assessment than echocardiogram. These techniques examine the tissue characteristics of the myocardium and quantify the extracellular volume, which is increased in myocardial fibrosis. One such method is T1 mapping of the myocardium both before and after the use of Gd contrast. Animal models106) and patients post-heart transplant and with DCM107) showed correlation between T1 mapping and myocardial fibrosis. Another technique used in CMRI is strain measurement. One such sequence uses MRI tagging, where a grid is created by MR pulses and the deformation measured in systole, but the principal image tracking method is different between CMRI and echocardiography.108)
Diagnostic Applications by Non-Invasive Imaging Studies
Duchenne Muscular Dystrophy
The primary pathological process in DMD cardiomyopathy is progressive myocyte loss with perturbed compensatory growth response and resultant myocardial fibrosis (Fig. 2). Significant changes in SF and EF tend to occur during adolescence in DMD patients. With the advancement in respiratory support of this group of patients and their longer survival, cardiomyopathy has become the leading cause of death.109) Due to limited mobility of DMD patients, overt symptoms of congestive HF are not recognized until the advanced stages of cardiomyopathy.
Ryan et al. measured SF and circumferential strain by transthoracic echocardiogram in a group of young (<8 years of age) patients with DMD and a control group and reported significant changes in the circumferential strain values in the DMD group compared with the control group at mid-ventricular anteroseptal, inferior, and infero-lateral segments, which could be a marker of subclinical cardiac disease in this group of patients starting in the first decade of life.110) Markham et al. compared diastolic function parameters between patients with DMD (<15 years of age with no HF) and controls. They assessed different diastolic function parameters, including Doppler-derived mitral E/A ratio, tissue Doppler-derived E′/A′ ratio, E/E′ ratio, IVRT, and mitral valve deceleration time. In this study, DMD had significantly worse findings overall on their diastolic function indices; patients who developed HF at follow-up had even worse diastolic function parameters at initial assessment compared with those who continued to have no manifestations of HF, signifying the importance of diastolic function abnormalities as a marker for future development of HF in young DMD patients.111) Another study by Spurney et al. showed that patients with DMD had significantly higher mitral A-wave velocities, lower E/A ratios, and lower Doppler tissue imaging mitral lateral E′ velocities when compared with the age-matched control subjects, indicating impaired diastolic function. In addition, the same study revealed that speckle-tracking derived myocardial strain and strain rate values (both longitudinal and circumferential) were significantly different in the DMD group compared with controls. The differences were notably significant, even in patients younger than 13 years with normal SF and normal MPI values.112)
Strain analysis in 19 DMD patients and 16 controls revealed significantly lower global circumferential strain (GCS) (−14.7±4.7 vs −23.1±2.9, p=0.001) and GLS (−13.6±5 vs −18.8±3, p=0.001) than the controls, suggesting that occult cardiovascular dysfunction was present.113) Circumferential strain was reduced in DMD patients compared with controls, even at a young age when other systolic function parameters were still normal, and worse strain values were noted in patients with decreased EF.114) Similar results were obtained by Ashford et al. in DMD patients.115) Hagenbuch et al. studied circumferential strain in DMD patients over a mean period of 15 months and found progressive decrease in strain values over time in all patients.116) Strain and strain rate have also detected early changes in cardiac function in adolescent patients with type 1 diabetes, in asymptomatic children with LV noncompaction and normal EF, and in heart transplant patients during an episode of rejection.117–119) While strain is clearly promising for the detection of subclinical and mild myocardial dysfunction, challenges include reproducibility of measurements and intervendor differences.120)
The diagnostic value of CMRI has been emphasized in detection of preclinical HF in DMD. In a small study involving 10 patients (ages 7 to 18 years) with DMD or Becker muscular dystrophy (BMD), Silva et al. investigated myocardial fibrosis by LGE-CMRI. Fibrosis was found in 70% of the patients tested, and those patients with fibrosis had significantly lower LVEF and higher LVESV.39) Of note, only two patients had abnormal findings on echocardiogram, signifying the importance of LGE in early detection of cardiomyopathy in muscular dystrophy. Soslow et al. compared T1 values after Gd contrast administration between patients with DMD and controls and found that DMD patients had shorter post-contrast T1 values compared with controls, even those patients without LGE or reduced EF.121) In a larger study on patients with DMD, Tanden et al. retrospectively reviewed the association of LGE to LVEF, rate of decline of EF, and effect of treatment with steroids.122) This study included 98 patients with DMD who had four or more CMRI studies finding that the age of onset of LV dysfunction was variable. This study showed that the rate of decline of LVEF in these patients increased after development of fibrosis on LGE imaging, and EF decline correlated with number of segments affected. They also found that longer duration of steroid treatment may decrease the rate of new onset fibrosis.122) Studies in adults with ischemic heart disease showed that LGE on CMRI is a better predictor of inducible monomorphic ventricular tachycardia than EF123) and development of major cardiac events and cardiac mortality.124) More studies are needed to evaluate the impact of LGE in DMD on prognosis and outcome. The limitations of LGE include the semiquantitative nature of the sequence and limited ability to assess for scarring in the presence of diffuse myocardial fibrosis.
Anthracycline-Induced Cardiotoxicity
Among those who survive their malignancy, cardiotoxicity is the third leading cause of morbidity and mortality, following relapse of primary malignancy and occurrence of secondary cancer.125) Central pathogenesis of AIC may be outlined by direct cardiomyocyte impairment causing myocardial thinning and ventricular dysfunction and premature senescence affecting endothelial cells and other cell types (Fig. 2). Cardinale et al. showed, in an adult study of AIC, that earlier treatment of HF is associated with a more favorable response to HF therapy and lower rate of cardiac complications.126) Earlier studies showed that pediatric patients who received anthracycline chemotherapy demonstrated acute decrease of systolic and diastolic function measurements immediately after chemotherapy; although the values remained within normal limits.127) However, the decline in LV systolic function is not a sensitive or reliable marker for early myocardial deterioration by AIC.128) It is essential to detect AIC in the preclinical stage to prevent long-term irreversible adverse cardiomyopathy.
Mavinkurve-Groothuis et al. showed that all myocardial strain parameters decreased during chemotherapy and the degree of decrease was proportional to the cumulative anthracycline dose despite normal SF in these patients. The changes in the strain parameters persisted when other biomarkers of cardiac damage such as troponin T level did not predict abnormalities in the strain.129) In one study, 71 children exposed to anthracycline chemotherapy were found to have diminished longitudinal and circumferential echocardiographic strain and particularly diminished diastolic strain rate despite having normal SF.130) Cetin and colleagues measured conventional echocardiographic parameters and strain in 45 childhood anthracycline-treated cancer survivors and age-matched controls. Both groups had normal EF, SF, and brain natriuretic peptide levels; the anthracycline group had significantly lower longitudinal and radial strain values.131) Poterucha et al. compared two-dimensional speckle-tracking echocardiography-derived longitudinal peak systolic strain (LPSS) values in adolescent patients receiving anthracycline chemotherapy and demonstrated small but significant changes in LPSS values at 4 and 8 months post-chemotherapy, compared with pre-chemotherapy and controls, that preceded the decline in EF.132) Comprehensive echocardiographic assessment, including three-dimensional (3D) LVEF, global longitudinal and circumferential myocardial strain, and diastolic function in 1820 adult survivors of childhood cancer, revealed that abnormal GLS and diastolic function were more prevalent than reduced 3D LVEF.128) However, current guidelines for AIC surveillance are heavily dependent upon 2D echocardiographic assessment of LV systolic performance as a primary method.71, 133) The advanced echocardiographic methods may be incorporated into these guidelines.
Toro-Salazar et al. demonstrated that CMRI-derived abnormal myocardial characteristics and abnormal regional myocardial function were detected in pediatric cancer survivors with normal LV systolic function, suggesting that CMRI parameters, LV peak circumferential strain, T1 mapping-derived relaxation time, and extracellular volume (ECV), were effective in detecting occult AIC.134) In comparison with echocardiogram, CMRI not only demonstrated higher incidence of reduced EF among 114 adult survivors of childhood cancer, but also more frequently identified preclinical LV dysfunction in previously undiagnosed survivors.135) Tham et al. studied late cardiotoxic effects in 30 pediatric cancer survivors (age 15±3 years) and demonstrated that myocardial T1 values and ECV correlated well with cumulative anthracycline dosage, exercise capacity, and LV remodeling.136) On the other hand, in 91 adult cancer survivors with reduced EF (35±8%), CMRI-derived indexed LV mass showed strong correlation with the total anthracycline dosage and the incidence of major adverse cardiovascular events, but the incidence of myocardial fibrosis by LGE was infrequent in this study.137) Further studies are warranted to reliably identify the preclinical stage of AIC by noninvasive imaging modalities.
Management of Preclinical HF
Preclinical HF in the pediatric population has not been well studied and unfortunately is not recognized until it progresses to an advanced stage with clinically overt symptoms. Guidelines from both European and United States cardiology societies do not provide specific recommendations for management of preclinical HF.138, 139) The ultimate goal of HF therapy is to improve hemodynamics, prevent disease progression, maintain quality of life, and allow optimal growth and development in these children, but currently available conventional HF therapy has very limited capacity. Most of the current recommendations are extrapolated from adult guidelines, as we commonly see in pediatrics. Within the field of pediatric HF, angiotensin-converting enzyme inhibitors (ACEi) are considered first-line of therapy and β-blockers are second-line. Anti-mineralocorticoids are also accepted in the treatment of pediatric HF,140) whereas diuretics are recommended only to be used to achieve a euvolemic status.141)
Duchenne Muscular Dystrophy
Cardiac dysfunction is a well-known and important complication of some neuromuscular disorders, especially in DMD.37, 43, 142–145) The cardiac status of DMD patients is difficult to assess clinically given their musculoskeletal and respiratory limitations. A study published in 2005 evaluated the effect of perindopril in patients with DMD with normal baseline EF, which demonstrated that early treatment, before the presence of symptoms and between the ages of 9 and 13 years, can delay the onset and progression of clinically-apparent LV dysfunction in children with DMD.146) Thus, recognition of the preclinical stage and early treatment appear critical for favorable outcome.
Cardioprotective treatment of preclinical cardiomyopathy in DMD has been widely advocated in recent years.10, 147) Previous studies have shown some benefit from ACEi in patients with DMD.148, 149) A study led by Viollet showed overall improvement in LV function in patients treated, but there was no significant difference between patients treated with an ACEi alone or in combination with a β-blocker.150) A small, randomized, double-blind trial of lisinopril or losartan in 22 patients showed equal effectiveness in improving LVEF over a year of observation by echocardiogram.151) β-blockers are reported to be beneficial when used in combination with ACEi.152) Despite the lack of strong evidence, the International Society of Heart and Lung Transplantation (ISHLT) expert panel recommended on their guidelines that ACEi therapy should be considered for DMD unless there is a specific contraindication153); although the optimal age of institution of therapy is not clearly delineated.
Since the benefit of preventive therapy has not been clearly proven, it is challenging to decide the timing to initiate cardiac pharmacotherapy in this complex and heterogeneous population.154) On the other hand, oral corticosteroids are commonly prescribed early with the goal of preserving skeletal muscle strength and pulmonary function.155) Multiple mechanisms have been proposed for the beneficial biological role of steroids in DMD myopathy, including nuclear effect via activation of calcineurin/nuclear factor of activated T cells (NF-AT) pathway, enhancement of proliferation of myogenic precursor stem cells, reduction in the rate of muscle breakdown, and direct transcriptional modifiers to increase synergistic molecules, i.e., utrophin.156) A study evaluating 462 boys with DMD concluded that patients treated with corticosteroids can have a delayed onset of cardiac dysfunction and up to a 20% lower likelihood of developing cardiomyopathy compared with untreated patients.157) Schram et al. demonstrated a positive impact of steroids in mitigating the development of DCM and mortality in 87 patients (mean age 9.1±3.5 years) followed for more than a decade.158) However, significant adverse effects of steroids need to be closely monitored.
A comprehensive and multidisciplinary approach is required to provide patients with optimal prevention, monitoring, and treatment strategies. Currently, a randomized, multi-center, placebo-controlled clinical trial has been initiated in the United Kingdom to investigate whether the introduction of ACEi (perindopril) and β-blocker (bisoprolol) before the onset of identifiable LV systolic dysfunction can attenuate the development of cardiomyopathy in DMD patients aged 5 to 14 years.159)
Anthracycline-Induced Cardiotoxicity
Chemotherapy-induced cardiotoxicity, most commonly caused by anthracyclines, can be silent initially but take years or decades to manifest as cardiomyopathy, HF, myocardial infarction, myocarditis, or other significant clinical cardiac dysfunction.70, 160) There is no consensus regarding prevention or treatment of asymptomatic patients with AIC, and patients with cancer are often excluded from large HF trials.161) The underlying mechanisms of AIC are poorly understood, but there are a number of pathological processes proposed by multiple investigators, as discussed earlier.
Various agents have been proposed for the prevention of cardiomyopathy due to AIC.56) A meta-analysis by Kalam et al. showed that different agents such as dexrazoxane, statins, ACEi, and β-blockers may all have a cardioprotective effect.162) Dexrazoxane prevents AIC not only by chelating redox-active iron and subsequently reducing ROS formation, but also by reducing anthracycline-induced DNA damage via topoisomerase 2-α and topoisomerase 2-β.163) Cardinale et al. reported the benefits of ACEi in patients treated with anthracyclines.126, 164) In adult patients with acute myocardial cell injury after high-dose chemotherapy, early treatment with ACEi demonstrated significant protective effects against LV systolic dysfunction (LVEF: 62.4±3.5% and 48.3±9.3% in ACEi and non-treated group, respectively).164) Complete recovery of the LV systolic function was observed in 64% of the patients when ACEi was initiated soon after therapy, whereas the cardioprotective effect was significantly diminished after 12 months of the chemotherapy.126) A well-designed double-blind, placebo-controlled study was conducted with the aim to test if ACEi would decrease the LV end-systolic wall stress (LVESWS) and therefore improve or prevent cardiac dysfunction.165) The study showed decreased LVESWS by ACEi, but the reduction was not associated with significant changes on LVEF or LVSF, and there were more side effects in the treated than the untreated group. The most recent pediatric HF guidelines from ISHLT have no specific recommendation for ACEi therapy in stage A HF, whereas they recommend routine use of ACEi for the treatment of asymptomatic LV dysfunction (HF Stage B) unless there is a specific contraindication.153) The decision to extrapolate these results and routinely treat patients with subclinical HF with ACEi requires careful consideration given possible side effects that could outweigh potential benefits.
Initial studies have shown that β-blockers can provide a significant cardioprotective effect on both LV systolic and diastolic function.166, 167) The cardioprotective effects of β-blockers are thought to be due to increased pro-survival signaling via recruitment of β-arrestin and transactivation of epidermal growth factor receptor (EGFR), mitigation of oxidative stress, and prevention of myocardial calcium overload, resulting in enhanced lusitropy,56) in addition to reduction of myocardial workload through negative chronotropic and inotropic effects. Carvedilol, a non-selective β-blocker, has been used to treat cardiotoxicity and has improved LV function and mortality in adults. The evidence in pediatrics is much more limited. A small prospective randomized control trial, called the OVERCOME trial showed an absolute difference of 3.1% in LVEF in patients being treated with carvedilol and enelapril compared with placebo.168) Other studies have shown a similar protective effects in patients treated with β-blockers.161, 169) One could recommend a slow titration of this therapy, but the evidence remains limited.
There is still no clear evidence to define whether prophylactic cardioprotection is effective in preventing progression of cardiomyopathy in pediatric cancer survivors, or whether healthy life style and exercise can help prevent myopathic changes in the heart. Although there are no published large human clinical trials, evidence from numerous animal studies suggests that aerobic exercise training is protective against AIC.170, 171) In a small prospective study in 21 long term childhood acute lymphoblastic leukemia survivors with normal EF, home-based exercise improved diastolic function indicated by TDI and peak circumferential systolic and diastolic strain rates.172) Aerobic exercise may modulate cardiotoxicity by mitigating oxidative stress, pro-apoptotic signaling, ultrastructural changes secondary to calcium overload, and energy metabolism alteration, and by enhancing protein synthesis.173, 174) While counseling healthy lifestyle for these patients is warranted, there is a need for new trials that assess the effects of healthy diet, exercise, and prophylactic cardiac medical therapies on cardiac morbidity and mortality in this high-risk population.
 ,Rami Kharouf,Adriana C. Prada-Ruiz,Jeanne M. BaffaTakeshi Tsuda
,Rami Kharouf,Adriana C. Prada-Ruiz,Jeanne M. BaffaTakeshi Tsuda