Primary cardiac tumors in infants and children are extremely rare; hence, there is very little literature available, and most knowledge is based on collections of case reports.1) Individuals with Down syndrome have an increased risk of developing several medical conditions. No prior report matches this description of a rare combination of cardiac fibroma and Down syndrome in pediatric patients. Here, we report the case of a neonate who had Down syndrome with cardiac fibroma, and we discuss the most appropriate way of making a diagnosis and treatment in patients with cardiac masses.
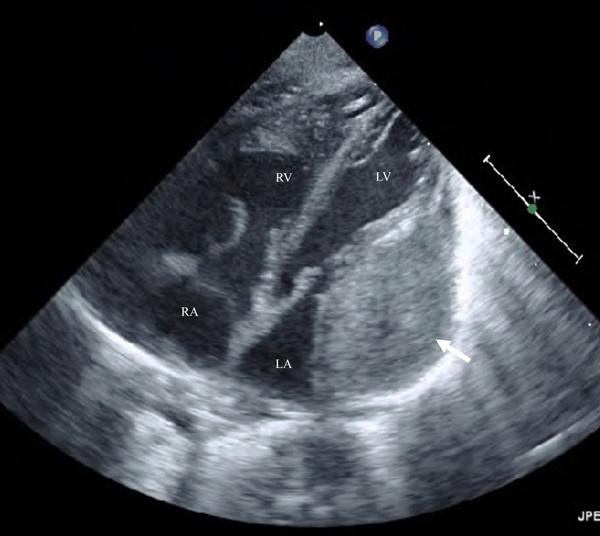
A 37-year-old pregnant woman in the 36th week of gestation (gravida 1, para 0) was transferred to our hospital due to a fetal cardiac mass noted during fetal echocardiography. Her fetal echocardiographic examination showed a large homogeneous, hypoechoic mass (24.0×16.7 mm), occupying the left ventricular cavity almost completely (Fig. 1). Other cardiac abnormalities were not detected. A male neonate was born via uncomplicated vaginal delivery at 36 weeks and 4 days of gestational age, weighing 2,896 g, the 1- and 5 minutes Apgar scores both 8. At birth it is found crying vigorously and spontaneously with good cardiorespiratory adaptation, tone and reactivity appropriate for gestational age. On physical examination, blood pressure was 58/34 mmHg, pulse regular with a rate of 132/min, breathing rate 54/min, transcutaneous oxygen saturation 94% in room air, and body temperature of 37.2°C. The initial cardiac examination revealed no significant murmur and typical facies associated with Down syndrome. Genetic testing confirmed karyotype 47, XY+21. Laboratory data, including plasma level of brain natriuretic peptide (BNP) and cardiac enzymes levels, were unremarkable. The plasma BNP level was 94 pg/mL (normal, <18.4 pg/mL). An electrocardiogram demonstrated sinus rhythm, right axis deviation, and low QRS voltage in V 5-6. A chest X-ray was negative for cardiomegaly with a cardiothoracic ratio of 0.59 but revealed a mild prominent bulge on the left cardiac border. Echocardiography revealed a large, solitary, homogenous mass contiguous with the left ventricular free wall and the left atrial wall, remarkably without evidence of ventricular systolic dysfunction (Fig. 2). There was no left ventricular inflow or outflow obstruction by Doppler interrogation. A chest contrast-enhanced Computed tomography (CT) showed a well-defined, homogenous, hypodense lesion bulging into the left ventricular and atrial cavity. No foci of calcification were identified. In addition, a CT scan of the head showed no evidence of calcification. Magnetic resonance imaging (MRI) of the chest showed a single large isointense mass in the left ventricular free wall on T1- and T2-weighted imaging. The solid component of the mass exhibited a slight enhancement following gadolinium administration (Fig. 3). Finally, these images summarized the signal intensity of nonspecific soft-tissue mass. Although we considered fibroma or rhabdomyoma would statistically be the most common etiology, tissue characteristics were not compatible with known benign or malignant masses.
The treatment approach was thoroughly discussed, before patient’s management aiming at better outcomes. Surgery was not indicated due to the lack of immediate risk of cardiac decompensation, life-threatening arrhythmias, intracardiac flow obstruction, and heart valve insufficiency. The parents were advised there was no absolute treatment strategy effective for cardiac tumor. The pros and cons of both surgical intervention and conservative treatment were carefully presented. The parents eventually elected to be treated conservatively unless the mass was classified as malignant. The parents agreed to accept open biopsy to confirm the histological diagnosis after a careful discussion regarding an increased risk of intraoperative and postoperative complications.
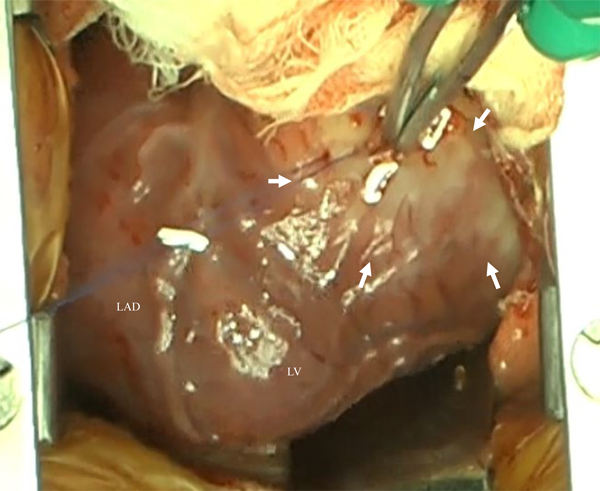
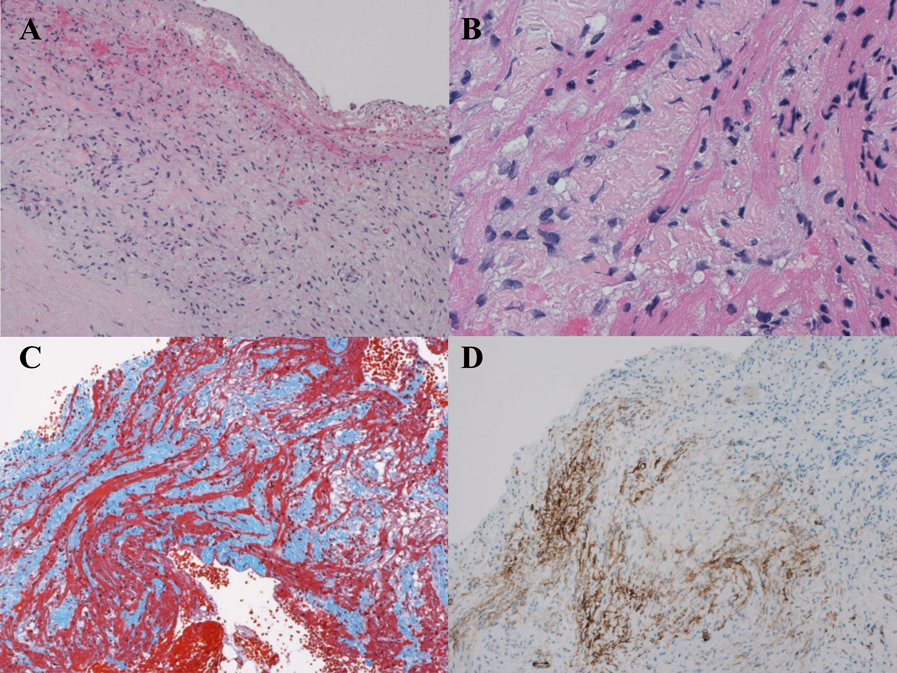
At 44 days of life, the patient was scheduled for open surgical biopsy to establish a diagnosis of the cardiac mass and determine whether it has malignant potential. Surgical open biopsy was performed through median sternotomy without cardiopulmonary bypass. A light yellow tumor appeared to originate from the left ventricular posterior wall near the base (Fig. 4). 3 biopsy specimens approximately 2–3 mm in size were obtained. Histopathologic examination demonstrated disarray of spindle cells with nuclei that appear to be normal (Fig. 5a, b) and increased amount of collagen fibers between cardiomyocytes (Fig. 5c). Immunohistochemical staining was positive for alpha-smooth muscle actin (Fig. 5d) but negative for desmin, CD31, and myogenin. The histological examination was compatible with a benign fibroma.
The patient was discharged on the 13th day following surgical biopsy with an uneventful postoperative course. Follow-up echocardiography shows normal left ventricular function and contractability with no evidence of obstruction. There have been no significant Doppler echocardiographic changes in mitral inflow since the foramen ovale closed. Furthermore, the cardiac mass remains virtually unchanged in size. The child is currently alive and well at 26 months of age.
Down syndrome is associated with a number of characteristic dysmorphic features and congenital or acquired medical problems.2) However, Down syndrome and cardiac tumor occurring in the same patient is a rare condition. In 2011 Ehara et al. showed the association with benign and malignant neoplasms in Down syndrome patients registered in the Annual of Pathological Autopsy Cases of Japan (1974–2000). In a total of 1514 cases with Down syndrome, there were eight cases with 10 benign tumors and 104 cases with malignant disorders, in which 87 cases with hematopoietic malignancies (83.7%) and 17 cases with solid tumors (16.3%), were identified.3) Interestingly, a combination of Down syndrome and cardiac tumor was not included in their report. Only a few cases of cardiac tumors associated with Down syndrome were published in the literature.4, 5) To our knowledge, this is the first case of cardiac fibroma in a patient with Down syndrome to be reported.
Primary tumors of the heart are uncommon in the fetus and neonate.6) The vast majority of primary cardiac tumours in children are benign, whilst approximately 10% are malignant.7) Cardiac fibroma is a rare, benign tumor that occurs predominately in infants and children.8) The tumors present in the neonatal period with cardiomegaly, murmurs, respiratory distress, cyanosis, arrhythmia, congestive heart failure, or a combination of these findings.6) Some individuals experience no apparent symptoms, while others may develop much more severe manifestations. The clinical manifestation of a fibroma mainly depends on its size and intracardiac location.9)
Currently, the improvement in imaging technologies not only allow the diagnosis of cardiac tumors as early as during fetal life but also help in planning surgery or follow up due to their quality of images.10) If a cardiac mass represents a tumour, its aetiology can often be determined by considering four factors; (1) the histology based likelihood; (2) the age of the patient at time of presentation; (3) the tumour location; and (4) non-invasive tissue characterisation. Using this approach, and integrating the clinical data, an accurate diagnosis and treatment strategy is usually possible without the need for open surgical biopsy.11) With MRI, fibromas are isointense relative to normal myocardium on T1-weighted images and are characteristically hypointense on T2-weighted images. With gadolinium-based contrast agent administration, fibromas generally show no contrast enhancement during perfusion imaging due to their avascularity. However, 7–10 minutes later, they classically show intense hyperenhancement on late gadolinium enhancement images. Additionally, lymphomas are typically homogeneous and isointense on T1- and T2-weighted images. Unlike other malignant tumors, there is generally minimal contrast agent uptake at late gadolinium enhancement. All tumors can have atypical appearances owing to altered tissue composition.12) Our patient’s MRI showed isointense on T1- and T2-weighted images with a slight enhancement. The MRI characteristics of the mass were nonspecific, with the differential diagnosis including both benign and malignant etiologies. Consequently, malignancy was not wholly excluded in our differential diagnosis. Based on this, in our patient surgical biopsy was recommended for confirmation.
Patients with primary cardiac tumors face an uncertain treatment strategy that ranges from conservative management to aggressive surgical intervention.13) In this case, the patient had a chromosome abnormality and remained totally asymptomatic with no echocardiographic evidence of hemodynamic important obstruction of inflow or outflow tracts, which made us hesitate to perform aggressive surgical treatment under cardiopulmonary bypass. There is a general agreement that surgical treatment should be performed whenever the cardiac mass is causing symptoms. Indication for surgical treatment remains controversial in patients who are strictly asymptomatic. In these patients, decision-making is challenging and should balance the risks of surgical treatment on one hand with the risks of conservative management on the other.14) While well-timed intervention is necessary, it is absolutely essential to avoid administration of wrong treatment which could potentially be lethal to the patient.15)
In this case, although the cardiac mass was large, the patient was asymptomatic. We realized that the surgical open biopsy would dramatically increase the surgical risk. Therefore, it might be possible to take a conservative approach with the cardiac mass, waiting until has increased in size. Although histologic and immunohistochemical examinations are useful to get a correct diagnosis of the type of tumor and its malignancy, clinicians should keep in mind that open surgical approach can have serious implications that require consideration. Primary cardiac tumors must be evaluated on a case by case basis, and flexibility is required to achieve a patient-centered outcome.
We report a rare case of cardiac fibroma in a newborn with Down syndrome. Due to the rarity of such cases, the appropriate way of making a diagnosis and treatment has not been conclusively determined. Conservative management of cardiac tumor in a newborn who is strictly asymptomatic seems to be an acceptable strategy when the risks of surgical intervention outweigh the benefits. Because of serious complications such as lethal arrhythmia and sudden death, close observation and informed consent are very important.
謝辞Acknowledgments
The author gratefully acknowledges Hiroki Mizukami, Professor, Department of Pathology and Molecular Medicine, Hirosaki University Graduate School of Medicine, for helping to obtain the histopathological images and analysis.
Conflicts of Interest
The authors declare that they have no conflict of interest.
引用文献References
1) Delmo Walter EM, Javier MF, Sander F, et al: Primary cardiac tumors in infants and children: Surgical strategy and long-term outcome. Ann Thorac Surg 2016; 102: 2062–2069
2) Roizen NJ, Patterson D: Down’s syndrome. Lancet 2003; 361: 1281–1289
3) Ehara H, Ohno K, Ito H: Benign and malignant tumors in Down syndrome: Analysis of the 1514 autopsied cases in Japan. Pediatr Int 2011; 53: 72–77
4) Krapp M, Baschat AA, Gembruch U, et al: Tuberous sclerosis with intracardiac rhabdomyoma in a fetus with trisomy 21: Case report and review of literature. Prenat Diagn 1999; 19: 610–613
5) Okada K, Masuoka A, Hotoda K, et al: A rare case of pediatric primary cardiac tumor in a patient with Down syndrome. Asian Cardiovasc Thorac Ann 2017; 25: 630–632
6) Isaacs H Jr.: Fetal and neonatal cardiac tumors. Pediatr Cardiol 2004; 25: 252–273
7) Uzun O, Wilson DG, Vujanic GM, et al: Cardiac tumours in children. Orphanet J Rare Dis 2007; 2: 11
8) Burke AP, Rosado-de-Christenson M, Templeton PA, et al: Cardiac fibroma: Clinicopathologic correlates and surgical treatment. J Thorac Cardiovasc Surg 1994; 108: 862–870
9) Navarini S, Latzin P, Kadner A, et al: Giant cardiac fibroma: An unusual cause of failure to thrive. Pediatr Cardiol 2013; 34: 1264–1266
10) Beroukhim RS, Prakash A, Buechel ER, et al: Characterization of cardiac tumours in children by cardiovascular magnetic resonance imaging: A multicenter experience. J Am Coll Cardiol 2011; 58: 1044–1054
11) Bruce CJ: Cardiac tumours: Diagnosis and management. Heart 2011; 97: 151–160
12) Motwani M, Kidambi A, Herzog BA, et al: MR imaging of cardiac tumors and masses: A review of methods and clinical applications. Radiology 2013; 268: 26–43
13) Elbardissi AW, Dearani JA, Daly RC, et al: Survival after resection of primary cardiac fumors: A 48-year experience. Circulation 2008; 118 Suppl: S7–S15
14) Pozzi M, Deux JF, Kirsch M: Conservative management of left ventricle cardiac fibroma in an adult asymptomatic patient. Int J Cardiol 2012; 161: e61–e62
15) Adam MA: The cardiac mass: Is it a thrombus, tumor or vegetation? Take it in the context of the disease. J Clin Diagn Res 2016; 4: 128