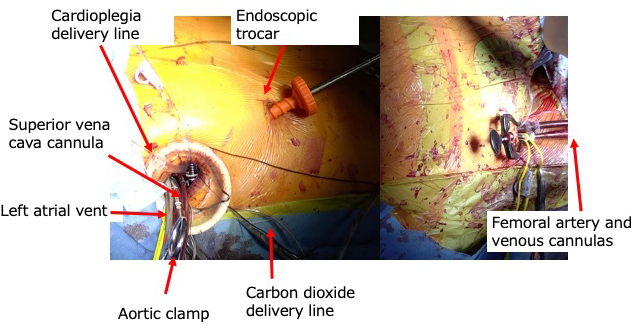
A seven-year-old female patient, diagnosed with ASD, was referred to our hospital. In the prior hospital, she underwent an esophageal echocardiogram to determine the possibility of catheter device closure. She was found to have an ASD with deficient inferior and posterior rims, deemed unsuitable for catheter closure. Therefore, she was referred to us for surgical closure. At our hospital, she underwent cardiac catheterization, which revealed a pulmonary-to-systemic blood flow ratio of 2.7, mean pulmonary arterial pressure of 18 mmHg, and pulmonary vascular resistance of 0.82 unit·m2. The ASD was 23 mm at its largest diameter, and the inferior rim was absent. The patient’s height and weight were 122.0 cm and 26.0 kg, respectively. During the operation, the patient was placed in the supine position with her upper body slightly lifted towards the left side. She was intubated using a double-lumen endotracheal tube. A vertical sub-axillary skin incision was made, and the chest was entered through the fourth intercostal space, where a wrap protector was placed. In between the protector and skin, a carbon dioxide delivery tube was placed. A skin incision was made along the inframammary fold to allow insertion of a 6-mm trocar for a 5-mm endoscope (ENDOEYE®, Olympus Corp., Tokyo, Japan). This incision was used for chest tube placement at the end of the operation. Then, a 1.5-cm skin incision was made at the femoral fold, and the external femoral artery and vein were exposed. After administration of heparin sodium, a 12-Fr straight aortic cannula (NextGen®, BioMedicus Inc. Eden Prairie, MN, USA) was inserted through the femoral artery into the external iliac artery. Subsequently, an 18-Fr straight venous cannula (PCKC-V®, Senko Medical Instrument Mfg. Co., Ltd., Tokyo, Japan) was inserted through the femoral vein into the inferior vena cava just below the diaphragm. After these procedures, the pericardium was opened, and a an 18-Fr straight venous cannula (TWN®, Senko Medical Instrument Mfg. Co., Ltd., Tokyo, Japan) was inserted through the right atrial appendage into the superior vena cava. The left atrial vent and aortic root cardioplegic cannulas were serially placed. The aorta was clamped, and the right atrium was opened. The intraoperative picture of the operative field is shown in Fig. 1. The ASD (2.5×1.5 cm) with a deficient inferior rim was closed directly using a 5-0 Prolene suture. After confirming the absence of leakage, the right atrial incision was closed using a 4-0 Prolene suture, and the aortic clamp was removed. After reduction of the cardiopulmonary bypass flow to 50%, all cannulas placed through the thoracotomy incision were removed. The pericardium was closed, leaving a sufficient window at the bottom, where a 15-Fr chest tube was placed. Until this time, all procedures were performed while the right lung collapsed. After resumption of two-lung ventilation, cardiopulmonary bypass was discontinued, and the femoral cannulas were removed. The myocardial ischemic, cardiopulmonary bypass, and operation times were 39, 137, and 250 min, respectively. She was then transferred to the intensive care unit in stable condition. She was weaned off from the ventilator and extubated two hours after the surgery. She was transferred to the general ward on day 2 and discharged on day 8. The intraoperative esophageal and immediate postoperative echocardiograms revealed an absence of an ASD leak. The length of skin incision was 1.5 cm (Fig. 2).
Presently, Amplatzer occluder device or other related device closure is the gold standard of treatment for atrial septal defects.1, 2) However, there still exist some patients who were identified to be a crossover group for surgery.3, 4) The factors of this crossover include a deficiency of the posterior or inferior rim and a large defect. This is a decisive moment of the patient’s life because the sternotomy skin incision scar can be a significant psychological burden. In consideration of this detriment, a right vertical infra-axillary mini-skin incision has been used for simple congenital heart defects. It can be performed without the aid of endoscopy, and its safety and efficacy as a treatment option have already been established.5) Apart from the excellent cosmetic results, it has been shown to have short recovery times.6) The length of the skin incision can be further minimized with the aid of endoscopy, and has been employed for simple congenital cardiac disease, such as atrial and ventricular septal defects as well as mitral valve surgery in young adults. Zhang et al.7) reported this technique for 27 patients with a mean age of 24.8 years, but the application of this technique for children has yet to be reported.
We achieved a single intercostal entry through a small skin incision which turned out to be less than two centimeters in length. The size is comparable with that in a report of minimally invasive endoscopic lobectomy for young patients with benign lung diseases.8)
One concern related to this procedure is lower limb ischemia by cannulation in the small femoral artery, which may result in lower limb compartment syndrome. To avoid this complication, the lower-limb muscle regional saturation of oxygen was monitored on the lateral side of the gastrocnemius muscle using an INVOS 5100C (Covidien Japan, Tokyo, Japan). The saturation was maintained above 55% throughout the procedure. Catastrophic bleeding event, while performing a standard cannulation for small child through a thoracotomy, is possible. We believe it safer to assure a circulation by using femoral artery. We think that the cardiopulmonary bypass, in a child with a low cardiac output, can be most safely conducted by using both femoral artery: thereby a smaller-sized cannula, compared with a single one, can be used. This was indeed our initial plan. In this case, however, the size of the right femoral artery was measured well above 4 mm, which was the size of the 12-Fr cannula (providing a full-flow for this patient). We believe that cardiopulmonary bypass can be safely conducted by selecting single or double femoral artery cannulas, individualized to each patient.
One problem, associated with an open-heart surgery thorough a thoracotomy, is an insufficient de-airing of the heart. In this case, de-airing was achieved thorough the cardioplegia needle hole after closing the atrium. Complete removal of the air was confirmed by transesophageal echocardiogram. As was already mentioned, a carbon dioxide delivery tube was placed inside the chest cavity. As a result, a ST-T segment elevation was not observed after removal of the aortic clamp.
The present case demonstrated that endoscopic minimally sub-axillary skin incision ASD closure is possible for patients as young as seven years of age However, this does not mean that visualization of the intrathoracic structures is as good as that in adults. It is known that a wide view is only accomplished if there is a wide free space for an endoscope to move freely. This is the reason why laparoscopic surgery necessitates intra-abdominal insufflation to create a surgical domain.9) The visualization of the ASD was, in retrospect, not excellent in this small patient. In this case, considering a cosmetic benefit, a 30°-angled endoscope was inserted from the future hole for the chest tube. It allowed excellent visualization of the aortic root. This is essential in mini-incision cardiac surgery because injuries of the left atrium or pulmonary artery by the aortic cross-clamp can be a reason for conversion to median sternotomy. In addition, bleeding control from the cardioplegia needle is crucial in the same procedure. However, we found that when the endoscope is inserted from the caudal portion to the thoracotomy, it does not allow visualization of the inferior part of the ASD, as it is hindered by the atrial wall. A lesson learned from this case was that the endoscope should be placed posterior to the main incision, at the similar intercostal level. By doing this, one could visualize almost entire operative filed including the atrial septal defect. This hole is still usable for the chest tuber placement.
 ,Taishi Fujii,Tamaki Takano,Shigeru SakamotoMakoto Ando
,Taishi Fujii,Tamaki Takano,Shigeru SakamotoMakoto Ando