Discrete subaortic stenosis (DSS) is rarely diagnosed during the fetal and neonatal stages of life. Many investigators consider DSS an acquired lesion that is possibly caused by excessive endothelial proliferation induced by shear stress resulting from abnormal blood flow through the subaortic tract.1, 2) We considered that DSS could be caused by congenital accessory tissue growth in the aortic valve.
We present the case of a 7-year-old boy (height, 106 cm; weight, 15.2 kg) born with multiple anomalies suggestive of the vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities (VACTERL) association. One day after his birth, he underwent radical repair of esophageal atresia and ventriculoperitoneal shunt insertion for hydrocephalus. At age 6 months, he underwent aortopexy through median sternotomy for tracheomalacia. At age 6 years, he underwent surgery to treat cryptorchidism. He was also being followed up for congenital scoliosis and short stature.
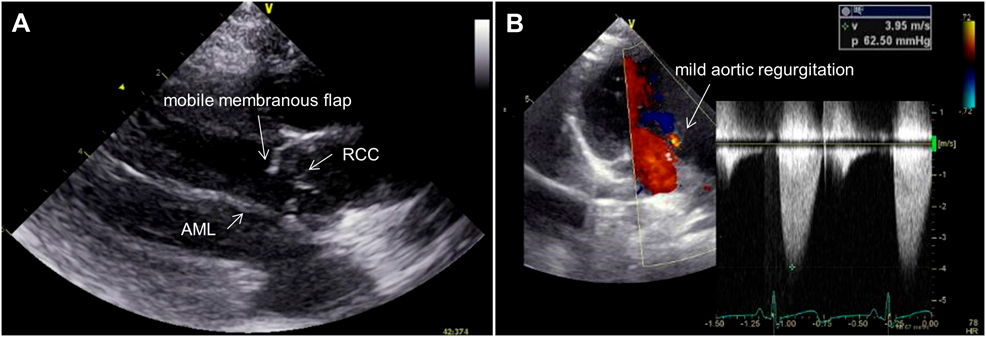
A systolic ejection heart murmur had been noted since infancy. A diagnosis of DSS was made because of a membranous structure detected by cardiac echocardiography. The flap length increased from 1.5 to 5.7 mm. The trans-DSS peak blood flow velocity increased from 1.7 to 4.0 m/s over the course of approximately 6 years, and mild aortic regurgitation developed (Fig. 1A, 1B; Supplementary Video S1). Cardiac catheterization revealed a resting peak pressure gradient of 40 mmHg between the left ventricle (LV) and ascending aorta (AAo), mild aortic regurgitation, and a persistent left superior caval vein. We considered the progression of DSS and newly developed aortic regurgitation as indications for surgical repair.
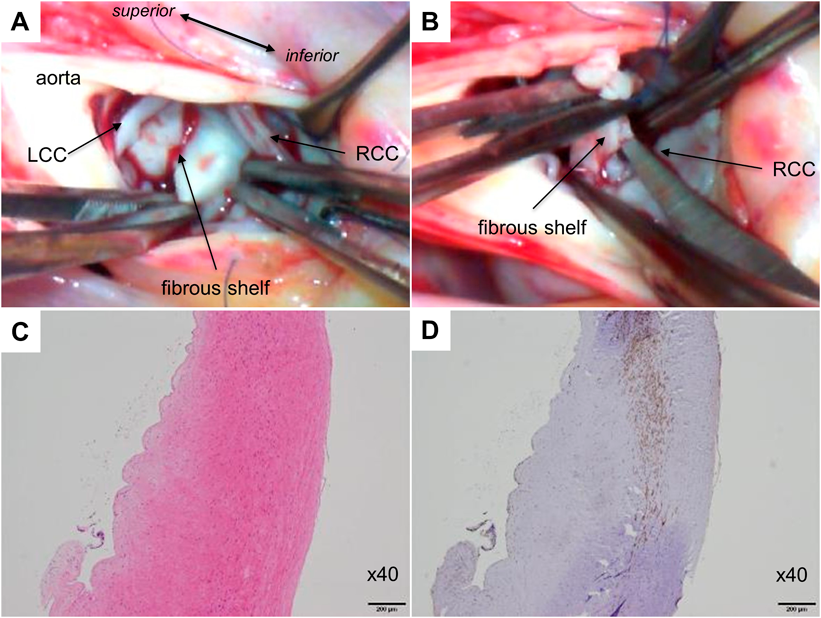
Re-sternotomy was performed and cardiopulmonary bypass was initiated using the ascending aortic and bicaval cannulation with left atrial venting. After the aortic cross-clamp was applied, the subaortic area was visualized through a transaortic approach. Closely related to three almost normal aortic valve cusps, a white thickening resembling two fused half-disk shapes was observed to form a fibrous shelf, extending from the center of the left coronary cusp to the right coronary cusps (Fig. 2A; Supplementary Video S1). This “bi-valved” shelf was carefully resected to avoid cusp injury (Fig. 2B).
Hematoxylin and eosin-stained sections of the specimen indicated fibrous connective tissue with an organized collagen fiber structure (Fig. 2C). Smooth muscle actin-stained sections showed evidence of a constructed layer of smooth muscle cells in the resected tissue (Fig. 2D). No cardiomyocytes or chordae-like structures were observed (Fig. 2C, 2D). Based on the gross and microscopic findings, the resected flap was likely an accessory aortic valve, and not just reactive tissue caused by shear stress. Postoperative transthoracic echocardiography indicated that the trans-LV-AAo peak blood velocity decreased to 2.0 m/s and aortic regurgitation remained mild. Two years have passed since the operation, and the patient has been kept under close medical follow-up.
Feigl et al. performed a pathologic study and reported that 16 DSS cases had aortic valve cusp involvement. These cases followed the pattern of the most common type of DSS, wherein fibroelastic tissue extends toward the aortic cusps.1, 3) In most cases, the tissue was found between the aortic valve and the anterior leaflet of the mitral valve, thus making it difficult to pathologically determine whether the flap of tissue in DSS was derived from the aortic valve, the mitral valve or ventricular muscle between the two valves.4) In this case, a membranous flap on the opposite side of the anterior leaflet of the mitral valve had been noted since infancy, and the pathological evaluation showed its structure to be similar to that of a valve. During the sixth to seventh weeks of the embryonic period, the primordia of the seminal valves on the right and left truncus swellings grew. They then fused to separate the truncus root and developed into the right and left coronary cusps. Furthermore, a minor truncus swelling developed into a non-coronary cusp from the opposite side. Simultaneously, the tubercles hollowed out at the upper surface, forming a mature aortic valve.5) A developmental abnormality occurred during either fusion of the left and right aortic valve primordia or hollowing out of these mesenchymal tissues. This led to the formation of half circumferential tissue under the coronary cusps on the other side of the anterior leaflet of the mitral valve. Some cases of DSS involving the aortic valve are caused by the growth of a “congenital accessory aortic valve” instead of by degenerative changes in the intima of the aorta. Early surgical intervention with close patient follow-up will prevent degeneration of the native aortic valve.
謝辞Acknowledgments
We thank Prof. Yoshihiro Komohara from the Department of Cell Pathology, Graduate School of Medical Sciences, Kumamoto University, for comments regarding pathology.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Ethical Standards
Written informed consent was obtained.
Note
Supplementary movies are provided online for this article.
引用文献References
1) Friedland-Little JM, Zampi JD, Gajarski RJ: Aortic stenosis, in Allen HD, Driscoll DJ, Shaddy RE, et al (eds): Moss and Adams’ Heart Disease in Infants, Children and Adolescents. The Netherlands, Wolters Kluwer, 2016, pp1088–1089
2) Lampros TD, Cobanoglu A: Discrete subaortic stenosis: Acquired heart disease. Eur J Cardiothorac Surg 1998; 14: 296–303
3) Feigl A, Feigl D, Lucas RV Jr., et al: Involvement of the aortic valve cusps in discrete subaortic stenosis. Pediatr Cardiol 1984; 5: 185–190
4) Rosenquist GC, Clark EB, McAllister HA, et al: Increased mitral-aortic separation in discrete subaortic stenosis. Circulation 1979; 60: 70–74
5) Sadler TW: Cardiovascular system, in Langman’s Medical Embryology (14th edition). Philadelphia, Wolters Kluwer, 2019, pp201–204
 1,Koji Fukae1,Osamu Matsuo2Kunihiko Joo
1,Koji Fukae1,Osamu Matsuo2Kunihiko Joo