Despite Japan’s unprecedented declining birthrate and aging society, it is important to continue the enhancement and development of child medicine. In the Japanese Society of Pediatric Cardiology and Cardiac Surgery, which the authors belong to, pediatricians and internists involved in cardiovascular treatment and cardiac surgeons have teamed up with specialists in multiple fields, engaging together in pediatric cardiovascular treatment for children with cardiac diseases and their families. For the past several decades, pediatric cardiovascular treatment in Japan has made remarkable progress, establishing a leading position in the world. However, it is now on the verge of collapse, mainly in rural areas, due to the recent severe shortage of physicians as well as the uneven regional distribution of physicians and clinical departments (decrease in surgeons, pediatricians, obstetricians, and gynecologists). In fact, pediatric cardiac surgeons are called ‘threatened species’, and the near future may see a shortage of physicians who can perform surgery for congenital heart disease if no measures are taken. This is likely to lead to the collapse of pediatric cardiovascular treatment in Japan, unless new pediatric cardiac surgeons are trained. Consequently, the Japanese Society of Pediatric Cardiology and Cardiac Surgery has set up a Division of Surgical Training to launch a project to train the next generation of pediatric cardiac surgeons.
This study, as part of the project, administered a questionnaire to surgical members of the Japanese Society of Pediatric Cardiology and Cardiac Surgery to obtain information about the actual status of pediatric cardiac surgeons in Japan, including working environment and training conditions. This article reports the results of the questionnaire, analyzes the actual status, and examines how to train the next generation of pediatric cardiac surgeons in Japan.
Questionnaire for Training the Next Generation of Pediatric Cardiac Surgeons
Method
Questionnaire period: June 26, 2018 to August 6, 2018
Questionnaire method: Requesting 420 cardiovascular surgeons, active members of the Japanese Society of Pediatric Cardiology and Cardiac Surgery, to answer an anonymous web questionnaire.
Number of answerers: 176 (Men: 161; Women: 15; Mean age: 46.1 years; Answer rate: 42%)
Question items: 30 questions (Table 1)
Table 1 Questionnaire items| ☆ Your profile |
| Q1: Sex 1. Man 2. Woman |
| Q2: Age Years |
| Q3: Years after graduation |
| Q4: Are you affiliated with a university? 1. Yes 2. No |
| Q5: Board Certificated Surgeon Yes, No Board Certificated Cardiovascular Surgeon Yes, No Board Certificated Cardiovascular Instructor Yes, No |
| Q6: Do you have a PhD? Yes, No |
| Q7: Have you studied overseas? Yes, No |
| Q8: Region where you work 1. Hokkaido 2. Tohoku 3. Kanto-Koshin 4. Tokai 5. Hokuriku 6. Kinki 7. Chugoku 8. Shikoku 9. Kyushu |
| Q9: Institution where you work 1. University hospital 2. Specialized hospital (including cardiovascular disease center and hospital for children) 3. Public general hospital 4. Private General Hospital 5. Other institutions |
| Q10: Annual number of surgical cases for a congenital heart disease at the aforementioned institution (cases in JCCVSD) |
| 1. Less than 25 cases 2. 25 to 50 cases 3. 50 to 100 cases 4. 100 to 200 cases 5. 200 cases or more |
| Q11: Number of surgeons engaged in the pediatric cardiac surgical field at the aforementioned institution |
| Q12: Your position 1. Chief 2. Staff member 3. Specialist |
| ☆Your training condition |
| Q13: Number of surgical cases in 2017 (cases in JCCVSD) |
| 1. Less than 10 cases 2. 10 to 20 cases 3. 21 to 50 cases 4. 51 to 100 cases 5. 100 cases or more |
| Q14: Number of surgical cases in which you participated as an assistant in 2017 (cases in JCCVSD) |
| 1. Less than 50 cases 2. 50 to 100 cases 3. 100 to 150 cases 4. 150 to 200 cases 5. 200 cases or more |
| Q15: Number of cases of surgery you have performed thus far (cases in JCCVSD) |
| 1. Less than 50 cases 2. 50 to 100 cases 3. 100 to 300 cases 4. 300 to 500 cases 5. 500 cases or more |
| Q16: Number of surgical cases in which you have participated as an assistant thus far (cases in JCCVSD) |
| 1. Less than 100 cases 2. 100 to 500 cases 3. 500 to 1000 cases 4. 1000 to 2000 cases 5. 2000 cases or more |
| Q17: Experience of surgery |
| VSD closure Performed, Not performed PA banding Performed, Not performed |
| SP shunt Performed, Not performed TOF repair Performed, Not performed |
| Fontan Performed, Not performed CoA repair Performed, Not performed |
| TAPVC repair Performed, Not performed |
| Arterial switch operation Performed, Not performed |
| Norwood Performed, Not performed |
| ☆Your working environment |
| Q18: On-duty days per month (including working days outside the workplace and voluntary on-duty days). |
| 1. 0 day 2. 1 to 3 days 3. 3 to 5 days 4. 5 to 10 days 5. 10 days or more |
| Q19: Working hours per week (including working hours outside workplace) |
| 1. Less than 50 hours 2. 50 to 60 hours 3. 60 to 80 hours 4. 80 to 100 hours 5. more than 100 hours |
| Q20: About the actual training/working systems |
| 1. Extremely dissatisfied 2. Dissatisfied 3. Hard to say 4. Reasonably satisfied 5. Satisfied |
| Q21: Reason for the aforementioned answer |
| ☆Your opinion |
| Q22: About your future |
| 1. Highly anxious 2. Anxious 3. Hard to say 4. No anxiety 5. What will be will be |
| Q23: Reason for the aforementioned answer |
| Q24: About consolidation of institutions |
| 1. Required 2. Hard to say 3. Not required |
| Q25: Required: Please provide a comment about a method for the consolidation of institutions. |
| Q26: What is required for training future pediatric cardiac surgeons is |
| 1. centers for training the next generation of pediatric cardiac surgeons (one or two centers throughout Japan). |
| 2. approved affiliated institutions for training the next generation of pediatric cardiac surgeons (less than 10 institutions). |
| 3. a system led by the Japanese Society of Pediatric Cardiology and Cardiac Surgery, enabling surgeons to perform surgeries overseas. |
4. Please describe another system for training and teaching if you have.
( ) |
| Q27: If centers or approved affiliated institutions for training the next generation of pediatric cardiac surgeons are established, you consider that the appropriate training period is |
| 1. 2 years |
| 2. 3 years |
| 3. 4 years |
| 4. 5 years |
| Q28: If centers or approved affiliated institutions for training the next generation of pediatric cardiac surgeons are established, you consider that the condition for entering them is |
| 1. permission of the chief at the institution which you belong to |
| 2. a guarantee of status during training |
| 3. a guarantee of salary during training |
| 4. a post after training |
| 5. a certification for training |
| 6. all of the aforementioned conditions |
7. another condition
( ) |
| Q29: About pediatric intensive care department |
| 1. Required 2. Hard to say 3. Not required |
| Q30: Please provide a comment on why you desired to become a pediatric cardiac surgeon. |
Results
1) Respondents’ Background
The 176 questionnaire respondents included 152 Board Certified Surgeons (86.4%), 133 Board Certified Cardiovascular Surgeons (75.6%), and 79 Board Certified Cardiovascular Surgical Instructors (44.9%). Of these, 164 belonged to a university (93.2%), 112 had a PhD (63.6%), and 84 had studied overseas (47.7%). They consisted of 76 chiefs of a pediatric cardiac surgical team (43.2%), 66 staff surgeons (37.5%), and 21 senior physicians in training (12%).
2) Working Environments of Pediatric Cardiac Surgeons
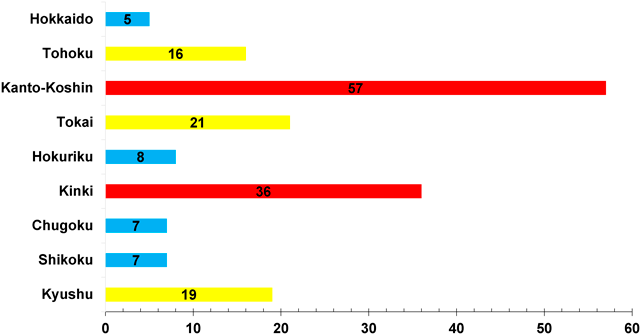
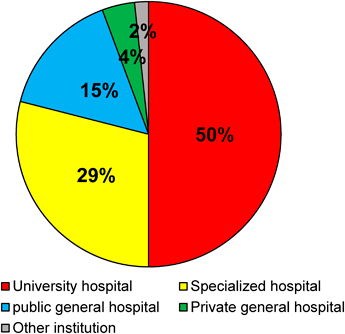
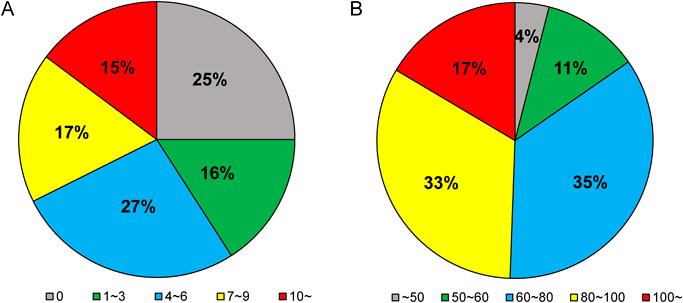
The most popular areas for pediatric cardiac surgeons in Japan were Kanto-Koshin (57 pediatric cardiac surgeons), followed by Kinki (36), Tokai (21), and Kyushu (19), and a small number of pediatric cardiac surgeons worked in Hokkaido, Hokuriku, Chugoku, Shikoku, and other local areas (Fig. 1). Their institutions included university hospitals (50%), specialized hospitals including hospitals for children and cardiovascular disease centers (29%), and public general hospitals (15%) (Fig. 2). Aside from specialized hospitals for children, an independent department of pediatric cardiac surgery is rarely found within a university or general hospital. Rather, two or three surgeons are engaged as a pediatric cardiac surgery team within the institution’s department of cardiovascular surgery, including a department of adult cardiovascular surgery. There is therefore a concern that pediatric cardiac surgeons are overworked. A total of 59% of the pediatric cardiac surgeons had four to six on-duty days per month, and 15% had 10 on-duty days per month or more. In addition, 35% worked for 60–80 hours per week, 33% for 80–100 hours per week, and 17% for more than 100 hours per week. Thus, 85% worked in excess of the statutory working hours (Fig. 3).
When questioned about the necessity of a pediatric intensive care department, 92% said it was ‘required’. Some pediatric cardiac surgeons at an institution with a pediatric intensive care department noted that postoperative intensive care provided by the cardiovascular intensive care department, reduced stress due to factors other than surgery.
3) Training Conditions of Resident Pediatric Cardiac Surgeons
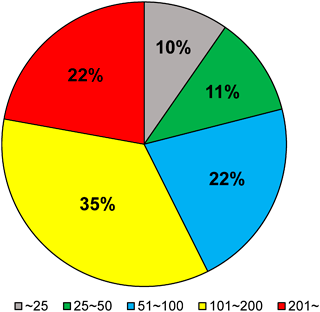
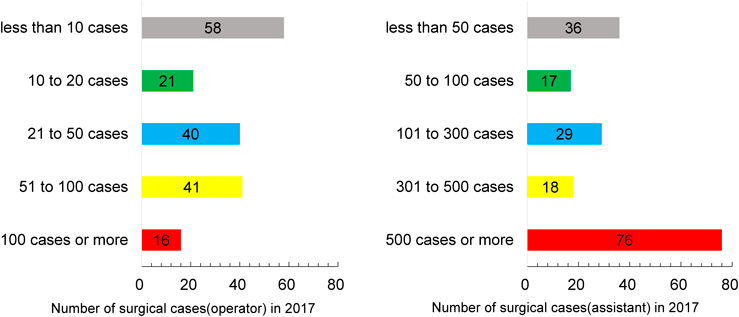
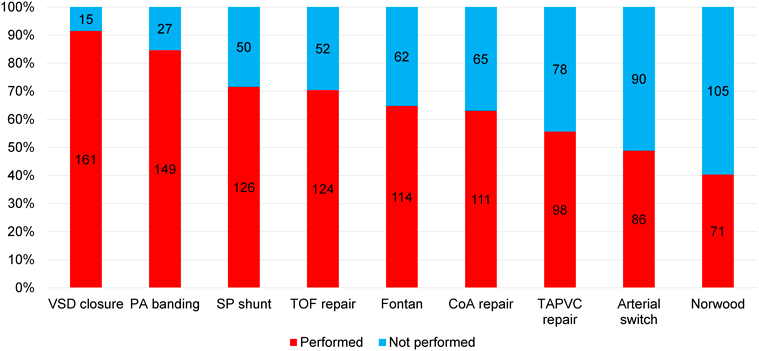
Of the surgeons, 22% worked at a so-called “high volume center” with 201 surgical cases per year or more, and 35% worked at an institution with 101 to 200 cases. On the other hand, 21% worked at an institution with 50 cases or less per year (Fig. 4). The number of surgical cases per surgeon was limited in such institutions. Of the questionnaire respondents, 58 performed less than 10 surgeries per year (33%), and 36 had performed less than 50 surgeries thus far (20%). Thus, it is difficult to state that they had performed an adequate number of surgeries (Fig. 5). Moreover, most difficult surgeries are performed by senior surgeons. For this reason, more than half of the surgeons answered that they had never performed difficult surgeries such as an arterial switch operation, or the Norwood operation (Fig. 6).
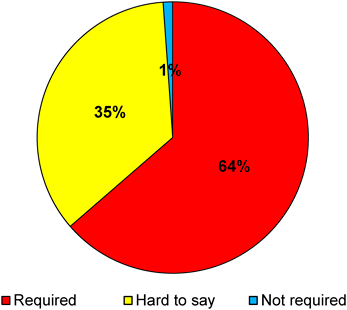
A consciousness survey was also conducted on the consolidation of institutions. While 64% answered that consolidation was ‘required’, 35% answered that it was ‘hard to say’ (Fig. 7). They presented various concrete strategies, which suggested that ‘consolidation of institutions’ raised many difficult problems.
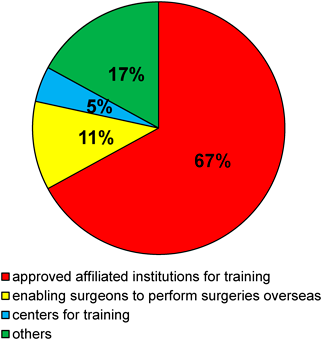
In response to a question about systems required for training the next generation of pediatric cardiac surgeons, the answers included the following: ‘approved affiliated institutions for training the next generation of pediatric cardiac surgeons’ (67%), and ‘system led by the Japanese Society of Pediatric Cardiology and Cardiac Surgery and enabling surgeons to perform surgeries overseas’ (11%) (Fig. 8).
4) Consciousness Survey on Pediatric Cardiac Surgeons
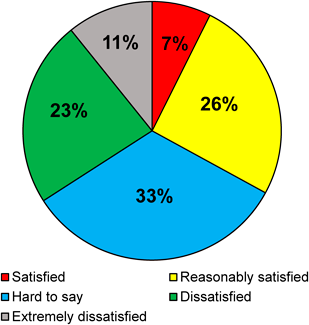
A survey was conducted on satisfaction with the actual working/training conditions. As a result, 33% answered that they were ‘extremely satisfied’ or ‘satisfied’, 33% answered that it was ‘hard to say’, and 34% answered that they were ‘extremely dissatisfied’ or ‘dissatisfied’. Thus, the answers were split almost evenly (Fig. 9). Some of the comments made are provided below.
- Reasons for answering that they were satisfied or reasonably satisfied:
- I am able to do the tasks I am requested.
- Although there are a few staff members, I feel the advantage of experiencing many cases.
- I have performed many surgeries and provided training as a chief.
- An appropriate number of staff members are responsible for a relatively high volume of cases.
- I am busy working but have active involvement in surgery as an operator or assistant for studying.
- I feel more fulfilled than tired.
- Reasons for answering that they were dissatisfied or a little dissatisfied:
- I have had obviously too few surgeries.
- The institution I belong to does not have enough cases allowing resident surgeons to perform surgery.
- I have to spend long off-duty hours at the institution and have an unreasonably low salary. Young physicians have too many on-duty days for postoperative management.
- I not only have too much clinical practice, but also have to work as a medical professor. I have a low salary.
- I have a few surgeries and am exhausted only by postoperative management and on-duty tasks.
Surgeons with many opportunities to perform surgery seemed to be highly satisfied, even if they were a little busy or had a slightly low salary. Meanwhile, the surgeons working at institutions with only a few cases had few opportunities to perform surgery, and were frustrated with spending their entire time conducting postoperative management and on-duty tasks due to the shortage of manpower. Young physicians do not want to work for such institutions, which has resulted in a vicious circle.
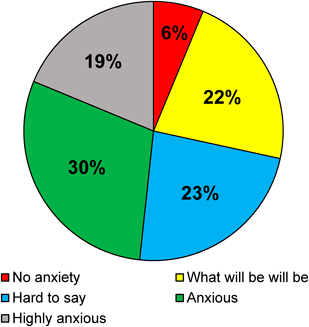
A survey was also conducted to determine whether the surgeons were anxious about their future. Of them, 19% answered that they were ‘highly anxious’, 30% answered that they were ‘anxious’, and 22% answered that ‘what would be would be’ (Fig. 10). Many comments have been provided, and some of them are described below.
- Reasons for answering that they were highly anxious or anxious:
- I wonder whether I can have a future in performing surgery, and whether the system making me overworked will remain unchanged.
- I do not know whether I can work as a surgeon in the future.
- I can see no future and do not know even whether I will continue to work at the Department of Pediatric Cardiovascular Surgery.
- I cannot work at the university hospital forever because of the term limit, and must make plans for the future. I am anxious about whether I can become an accomplished surgeon.
- I have seen many surgeons obtain a post of operator with effort, but are then compelled to quit the post for various reasons (such as poor performance and relationship with the department of internal medicine).
- I am anxious about the training of successors, and plans for my future after retirement.
- I am anxious about whether my team can remain the same in the future.
- My work is mentally and physically hard, and I wonder how long I can work with only a sense of responsibility and a spirit of self-sacrifice.
Not only resident surgeons, but also instructors are spending their days worrying.
The question, ‘why did they want to become a pediatric cardiac surgeon’, resulted in responses of impressive ideals and insights from the physicians engaged in this field. Some of the answers are provided below:
I have an academic interest in the pediatric cardiac surgical field, and it is rewarding to make children dramatically healthier.
I thought that if I became a pediatric cardiac surgeon, I could provide my skills and knowledge to treat children, contributing to their life and the well-being of their family.
I underwent surgery for a congenital heart disease, and my life was saved.
When I was a sixth-year medical student, I saw a child with Tetralogy of Fallot returning to the intensive care unit with pink-up after the surgery. This seemed to be a real miracle and I was quite moved.
Surgeons can save lives directly through surgery. However, it has recently been difficult to endure the pressure.
I have gradually started thinking that I will devote myself to treating children with congenital heart disease through contact with their family.
I want to save the lives of children who will bear the future. I want to save more lives.
I feel that it is rewarding that I can save the future of children.
I hope that children will spend their life enjoying some pleasures of life while occasionally experiencing pain and sadness, and I want to facilitate this.
When observing a surgery for a congenital heart disease, I was surprised with a drastic change in the hemodynamics, and I was fascinated by the beauty of each tissue. I gradually decided to specialize in the field of pediatric cardiac surgery. I naturally feel pressured about saving the life of children, but I think of it as a challenging job demand.
My surgery can provide children with time they would not have if the surgery was not performed, which is worth devoting my life to.
I knew from the beginning that pediatric cardiac surgeons would have difficult tasks and that efforts would not guarantee any future returns (such as position), but thought that the tasks were very challenging. As I believe that almost all physicians who desire to become pediatric cardiac surgeons are working with the same spirit, I wish that there would be a system rewarding effort and labor to some extent, although it is undeniable that surgical ability varies by individual.
Number of Physicians Engaged in the Field of Pediatric Cardiac Surgery
A congenital heart disease is a relatively common disease among infants and is observed in one out of every 100 newborns. In Japan, approximately 10,000 children per year are born with congenital heart disease. A congenital heart disease is a congenital cardiac structural abnormality, and almost all cases are indicated for surgical treatment. In Japan, surgery for a congenital heart disease is performed in approximately 9,000 cases per year, and this number has remained almost unchanged for the last 20 years, despite the declining birthrate.1)
Training future pediatric cardiac surgeons is essential to continue performing surgeries for congenital heart disease in 9,000 cases per year. However, the number of young surgeons engaged in the field of pediatric cardiac surgery has been decreasing. In recent years, various media have reported on the shortage of physicians in the departments of gynecology, obstetrics, and pediatrics, which has become a social issue. While various measures have slightly increased the number of physicians in these departments, it is still not enough. On the other hand, the number of surgeons has been steadily decreasing. Moreover, the age distribution of surgeons shows a high percentage of surgeons in their 40 s to 60 s, and a marked decline in the number of surgeons in their 20 s to 30 s.2) The mean age of the questionnaire respondents was 46.1 years, which showed that pediatric cardiac surgeons were no exception.
The number of members of the Japan Surgical Society was around 2,000 per year from the late Showa to the early Heisei era, when physicians in their 40 s to 50 s, currently playing an active and central role in surgical medical treatment, graduated from their university’s medical faculty. However, the number has fluctuated at around 700 per year in recent years. In the New Medical Specialty System initiated in 2018, the enrollment to the first surgical specialist training program was 805 across the country. Of the 805 members, the number of physicians who may be engaged in the field of pediatric cardiac surgery in the future was calculated to be less than 8 based on the number of Board Certificated Surgeons as of November 2018 (6,777 gastroenterological surgeons, 1,492 respiratory surgeons, approximately 130 pediatric cardiac surgeons of 2,194 cardiovascular surgeons, 557 pediatric surgeons, and 1,586 breast surgeons: Investigation of the web page of each society).
Of the 130 pediatric cardiac surgeons, most worked in Tokyo, Kanagawa, Shizuoka, Aichi, Osaka, Kyoto, Hyogo, and Fukuoka. One or two work in certain rural prefectures, while other prefectures have no pediatric cardiac surgeons. For this reason, the pediatric cardiac surgical treatment system is collapsing in some areas.
Working Environment of Pediatric Cardiac Surgeons
Pediatric cardiac surgeons work hard. Surgery in child patients with severe heart disease frequently lasts for many hours, requiring delicate procedures, and close and careful postoperative management. However, under current circumstances involving staff shortages, postoperative management is also performed by surgeons in Japan, resulting in severe overwork. The results of this questionnaire revealed that pediatric cardiac surgeons worked mainly at university hospitals, and a few surgeons were engaged in pediatric cardiovascular treatment at each institution. As pediatric cardiovascular treatment requires not only pediatric cardiac surgeons, but also a multidisciplinary team including pediatric cardiologists, neonatologists, anesthesiologists, obstetricians, clinical technicians, and nurses, treatment in this field can be provided exclusively at university hospitals, specialized hospitals, or some general hospitals. An independent department of pediatric cardiac surgery is rarely found at a university or general hospital; it can only be found at a specialized hospital for children. A department of pediatric cardiac surgery is normally present as a team in the department of cardiovascular surgery, including a department of adult cardiovascular surgery. In reality, two or three cardiac surgeons are engaged in the pediatric cardiac surgical field in most institutions. In some institutions, only one surgeon may be engaged. Furthermore, pediatric cardiac surgeons working at a university hospital have to be engaged in tasks other than pediatric cardiac surgical treatment, including teaching as a professor at the medical faculty, treating adult patients, and even working outside the university hospital to make up for their low salary. Therefore, it can be stated that the pediatric cardiac surgical setting is considerably shorthanded, and it is in danger of collapsing.
The overburdening of physicians is well known, and the necessity of reform has been discussed. As special management is required after pediatric cardiac surgery, it is frequently difficult for other physicians to take measures, and only a pediatric cardiac surgical team is placed on-call. According to the questionnaire results, 59% of the pediatric cardiac surgeons had four to six on-duty days per month, and 15% had 10 or more on-call days per month. Moreover, when a patient becomes serious, the attending physician must stay overnight for many days. Some pediatric cardiac surgeons may actually perform voluntary on-call work, which is not represented in this questionnaire. According to the questionnaire, 35% worked for 60–80 hours per week, 33% for 80–100 hours per week, and 17% for 100 hours per week or more. Thus, 85% worked in excess of the statutory working hours. It is no exaggeration to state that all pediatric cardiac surgeons, including department directors, professors, and hospital directors throughout Japan, are placed in a working environment that can cause death from overwork. Such an environment is naturally avoided by young medical students. It is impossible to attract young medical students with only ‘rewarding tasks’.
As described above, the current state is that postoperative management is also performed by surgeons in Japan. In response to the question about the necessity of a pediatric intensive care department, 92% answered that it was ‘required’. In a survey on satisfaction, some pediatric cardiac surgeons at an institution with a pediatric intensive care department commented that team medical care, in particular, postoperative intensive care provided by the cardiovascular intensive care department, reduced stress and the workload for surgeons. While there is no doubt that the establishment of a pediatric intensive care department will contribute to improving the working conditions for pediatric cardiac surgeons, there are still very few pediatric intensive care physicians throughout Japan. Such an establishment should be considered an important development for the future.
Training Conditions of Resident Pediatric Cardiac Surgeons
The superior skills required for pediatric cardiac surgery involves a long training period. Moreover, resident pediatric cardiac surgeons cannot always become full-fledged surgeons. Physicians who fail to become full-fledged surgeons while tolerating considerably harsh working conditions, and going through long and difficult training, may find themselves to be unmarketable. This naturally leads young medical students to avoid the field of pediatric cardiac surgery.
The results of this questionnaire confirmed that the training environments of pediatric cardiac surgeons differed greatly among institutions. While approximately half of the pediatric cardiac surgeons worked at institutions with 100 surgical cases per year or more, approximately 20% of the surgeons worked at institutions that had 50 surgical cases per year or less. Inevitably, the number of surgical cases per surgeon varied, and it is difficult to state that all pediatric cardiac surgeons have performed an adequate number of surgeries. Some pediatric cardiac surgeons perform less than 10 surgeries per year, and have performed less than 50 surgeries thus far. In addition, senior surgeons perform almost all difficult surgeries. However, the number and the difficulty level of surgeries varied greatly among the age groups, showing a wide difference depending on institutions. In other words, some resident physicians received training in a favorable environment, while others did not.
The questionnaire unsurprisingly showed that ‘satisfaction’ and ‘anxiety about the future’ also varied widely. In response to a question about ‘satisfaction’, the answers were evenly split into three categories: ‘satisfied’, ‘hard to say’, and ‘dissatisfied’. It can be stated that some respondents were ‘satisfied’ primarily because they had many opportunities to perform surgery. The majority of pediatric cardiac surgeons work at a university hospital, but they have many tasks other than treatment activities in their specialized field. Despite their low salaries, surgeons with many opportunities to perform surgery seem to be highly satisfied. According to the questionnaire on members aged 40 years or younger of the Japanese Society of Cardiovascular Surgery (private correspondence) conducted at around the same time as this questionnaire, the satisfaction of the actual pediatric cardiac surgical training was 3.25, on a five-point scale, and the surgeons working at an institution with 100 cases of pediatric cardiac surgery per year or more showed high satisfaction. On the contrary, the physicians working at an institution with a few cases were dissatisfied at performing too few surgeries, at their unreasonably low salary, at young physicians having too many on-duty days for postoperative management, and at being too busy with routine duties. Young physicians do not want to work for such institutions, which has resulted in a vicious circle.
Some complaints are understandable, but courage is required to dive into a field that could cause ‘anxiety about the future’. In fact, more than 70% of the pediatric cardiac surgeons were ‘anxious about the future’ in varying degrees, and only 6% answered that they had ‘no anxiety’. The questionnaire for surgeons aged 40 years or younger showed similar results. Moreover, even young surgeons receiving training with ‘high satisfaction’ were found to be ‘anxious about the future’. The respondents noted many anxieties, including: ‘Can I work as an operator, although difficult skills are required?’ ‘Can a system be established to train the next generation?’ It is presumed that young physicians engaged in the field of pediatric cardiac surgery will have the main tasks of surgical assistance, postoperative management, and ward tasks. Enormous courage is required for entering the pediatric cardiac surgical world, which does not secure the future of residents despite long-term training. It is necessary to establish a system that enables residents to have some prospects of success, and be free from anxieties. It is true that it is not easy to acquire the skills involved, however, it is undesirable to maintain the current status where the training environment varies depending on institutions. Instead, it is necessary to create a training environment where the number of surgical cases, difficulty, and other properties are programmed, to run a training facility independent of the university which a surgeon graduated from or belongs to, and to improve the harsh working environment. As many answerers mentioned in the questionnaire, it is necessary to dispose of the current system maintained by universities and their affiliated hospital and to establish an all-Japan system training the next generation.
As shown in many answers to the question, ‘Why did you desire to become a pediatric cardiac surgeon’, pediatric cardiac surgeons have rewarding tasks, including ‘directly saving the life of children’. It is necessary to create a system enabling young medical students with enthusiasm to become a pediatric cardiac surgeon filled with hopes and dreams to have fair training opportunities, and to mature into a pediatric cardiac surgeon playing an important role in Japan’s pediatric cardiovascular treatment.
謝辞Acknowledgments
We would like to express our deep gratitude to Dr. Akinori Hirano, Dr. Kenichi Okamura, Dr. Masashi Kabasawa, and physicians aged 40 years or younger from the Japanese Society of Cardiovascular Surgery for providing valuable answers to the questionnaire.
Conflicts of Interest
There is no conflict of interest to be disclosed in this article.
Originally published in Pediatric Cardiology and Cardiac Surgery, Vol. 35 (2019), No. 2, pp. 61–69