Total anomalous pulmonary venous connection (TAPVC) is a rare disease that accounts for approximately 1.5% of all congenital heart diseases. In the neonatal period, it is a typical example of a disease that requires urgent surgery. Although it has been reported that the postoperative survival is over 90%, the prognosis is poor in infants with postoperative pulmonary venous obstruction (PVO) with a mortality rate of approximately 50%.1, 2) The surgical outcome is particularly unsatisfactory in patients with heterotaxy syndrome associated with a functionally single ventricle. While early detection of PVO and reintervention might improve patients’ outcome, predictors of PVO following repair procedures remain unknown.3–5)
Our hospital introduced a 320-row multidetector computed tomography (CT) imaging system (MDCT) (Toshiba Medical Systems Corporation, Tochigi, Japan) in 2007. This equipment enabled CT scanning with a lower dose of radiation than the previous machine did. This study evaluated the characteristics of postoperative CT images in patients with TAPVC who underwent treatments at the Iwate Medical University Hospital.
The study was approved by the ethical board of the Iwate Medical University (MH2019-166) and information on the research was published on the homepage. In addition, participants were provided opportunities to withdraw from the study at any point in time.
Patients with TAPVC who received treatment at the Iwate Medical University Hospital during July 2012–December 2018 were included in the study, and their information was obtained from medical records. After the initial surgery, these patients were followed up at an interval of 1–6 months, and they underwent echocardiography for 2 years. Subsequently, they underwent annual evaluation. We included patients with TAPVC with uncomplicated congenital heart disease (e.g., atrial septal defect and patent ductus arteriosus), those with complicated congenital heart disease (e.g., a single ventricle and pulmonary atresia), and those with heterotaxy syndrome.6) Patients with chromosomal abnormalities were excluded.
We assessed sex, age at the initial repair, body height and weight, presence or absence of lower body weights, prenatal diagnosis, in-hospital births, the Cesarean section, perioperative death, TAPVC types, ventricular morphology, heterotaxy syndrome, pre- or postoperative PVO, surgical procedure (conventional or the so-called suture-less technique),7, 8) echocardiographic data, and contrast-enhanced CT findings.
TAPVC was classified into four types (i.e., supracardiac, cardiac, infracardiac, and mixed) based on the Darling classification.9) After the TAPVC repair, PVO was monitored by echocardiogram. PVO was defined as a condition where 1) ultrasonography demonstrated that blood flow velocity at the entrance of the left atrium was ≧1.6 m/s; or 2) the flow patterns were monophasic or continuous.10) During the study period, CT was performed in all cases approximately 3 months after surgery as our institutional protocol. Stenosis across the pulmonary vein (PV) in the CT image was defined on the basis of the radiologist’s reports where narrowest PV diameter was less than 50% of the distal PV (as a reference structure).
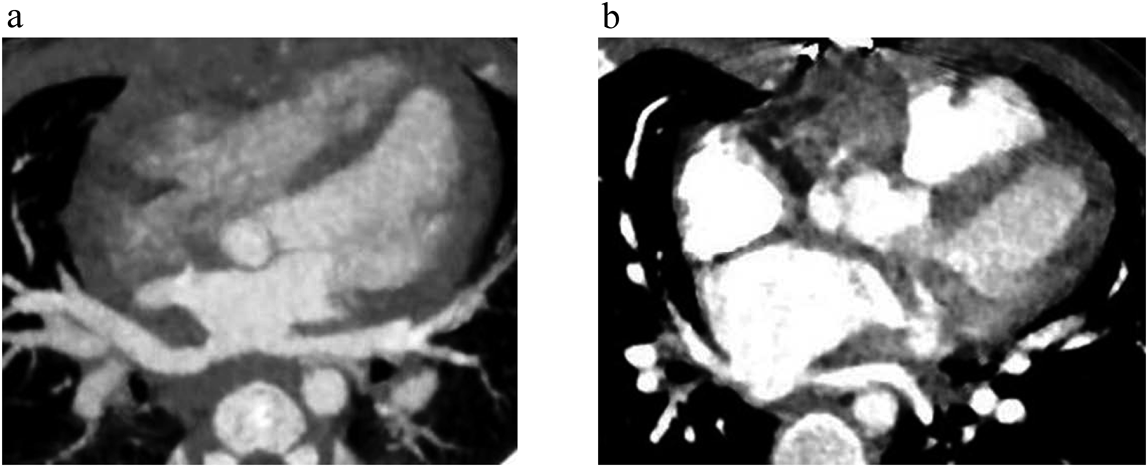
Orientation of the anastomotic site was classified into two categories. When the common PV and the atrium are anterior to the spine, the orientation was regarded as a central type. The other patter was named as a lateral type in which the anastomotic site was to the right or the left of the spine and the PV coursed in front of the descending aorta and the vertebrae. The anastomotic site was assessed on CT images by two researchers (HT and TT) (Fig. 1). Manifestations of pulmonary congestion was our indication for surgically relieving PVO.
Data were analyzed using IBM SPSS Statistics Grad Pack version 26.0 (SPSS Inc. Chicago, Illinois, USA). Patient characteristics were tabulated using the median, minimum and maximum values, counts, and percentage of categorical variables. The concordance rate for imaging evaluation was assessed using the K-correlation.
Patient Data (Table 1 and 2)
Table 1 Patients’ Characteristics| Variable | Number (%) or Median (Range) |
|---|
| Sex | |
| Male | 10 (56) |
| Female | 8 (44) |
| Age at surgery (day) | 19 (0–351) |
| Height at surgery (cm) | 48.5 (41.1–72.0) |
| Body weight at surgery (g) | 3015 (1600–8900) |
| >2500 g | 17 (94) |
| 2000–2500 g | 1 (6) |
| Fetal diagnosis | 4 (22) |
| Inborn | 6 (33) |
| Cesarean section | 8 (44) |
| Hospital death | 0 (0) |
| TAPVC type |
| Supracardiac | 3 (17) |
| Cardiac | 4 (22) |
| Infracardiac | 6 (33) |
| Mixed | 5 (28) |
| Univentricular heart | 4 (22) |
| Heterotaxy syndrome | 4 (22) |
| preoperative PVO | 10 (56) |
| Reoperation for PVO | 4 (22) |
| sutureless repair | 5 (28) |
| Age at CT (day) | 133 (33–556) |
| Radiation dose (mSv) | 0.65 (0.40–1.32) |
| PVO, pulmonary venous obstruction; TAPVC, total anomalous pulmonary venous connection |
Table 2 Characteristics of 18 patients who underwent 320-row multidetector CT| No. | TAPVC type* | age at surgery (day) | CT | echocardiography | reoperation | PVO site | operative finding |
|---|
| age (day) | radiation dose (mSv) | site of anastmosis | stenosis | age (day) | PV flow velocity (m/s) | continuous flow |
|---|
| 1 | 1b | 3 | 35 | NA | Central | No | 52 | 0.67 | No | No | | |
| 2 | 2a | 3 | 402 | 0.75 | Central | No | 382 | 0.91 | No | No | | |
| 3 | 2a | 16 | 121 | 0.54 | Central | No | 33 | 0.55 | No | No | | |
| 4 | 1a+3 | 157 | 182 | 1.32 | Central | No | 178 | 0.40 | No | No | | |
| 5 | 1a+3 | 4 | 74 | 0.57 | Central | No | 22 | 0.93 | No | No | | |
| 6 | 1b | 22 | 169 | 0.65 | Central | Yes | 175 | 0.70 | No | No | | |
| 7 | 3 | 68 | 150 | 0.81 | Central | Yes | 92 | 1.28 | No | No | | |
| 8 | 3 | 0 | 33 | 1.06 | Central | Yes | 18 | 0.60 | No | No | | |
| 9 | 3 | 1 | 83 | 0.40 | Central | Yes | 82 | 0.70 | No | Yes | LPV | Compression by DAo |
| 10 | 1a | 102 | 547 | 0.89 | Lateral | No | 561 | 0.85 | No | No | | |
| 11 | 2a | 13 | 556 | 1.15 | Lateral | No | NA | NA | NA | No | | |
| 12 | 2a | 71 | 85 | 0.51 | Lateral | No | 191 | 0.57 | No | No | | |
| 13 | 1b+2b | 337 | 407 | 0.64 | Lateral | No | 412 | 0.74 | No | No | | |
| 14 | 3 | 1 | 89 | NA | Lateral | Yes | 61 | 0.58 | No | No | | |
| 15 | 3 | 2 | 274 | 0.60 | Lateral | Yes | 183 | 1.22 | No | No | | |
| 16 | 1b+2b | 49 | 144 | 0.62 | Lateral | Yes | 69 | 1.28 | No | Yes | CPVC-LA | Intimal hyperplasia |
| 17 | 3 | 88 | 108 | 0.99 | Lateral | Yes | 108 | 1.04 | Yes | Yes | LPV | Compression by DAo |
| 18 | 1a+2a | 39 | 104 | NA | Lateral | Yes | 102 | 2.06 | Yes | Yes | LPV, RPV | Intimal hyperplasia |
| *TAPVC type Darling’s classification (1=Supracardiac, 2=Cardiac, 3=Infracardiac, 4=Mixed, a=left reflux, b=right reflux). DAo, descending aorta; PVO, pulmonary venous obstruction; TAPVC, total anomalous pulmonary venous connection |
A total of 22 patients were diagnosed as having TAPVC between July 2012 and December 2018. Among them, 4 patients were excluded from this study because one patient did not undergo TAPVC repair at our hospital and the other 3 did not undergo postoperative CT imaging due to their critical conditions. As a result, we evaluated 18 patients (10 male and 8 female). At the time of the initial repair, median age was 19 (0–337) days, with body height and weight 48.5 (43.0–65.0) cm and 3,015 (2,400–7,200) g, respectively. The body weight was less than 2,500 g at surgery in one patient. Prenatal diagnosis had been established in 4 cases, in-hospital birth was managed in 6, the Cesarean section was carried out in 8. TAPVC types were supracardiac (n=3), cardiac (n=4), infracardiac (n=6), and mixed (n=5). Heterotaxy syndrome with physiologically single ventricle was found in 4, preoperative PVO in 10, and reoperation for PVO relief was carried out in 4. The primary surgical procedure was by a conventional method in 13 and a suture-less method in 5.
Postoperative PVO Diagnosis Based on 320-Row MDCT
The median age at the time of postoperative CT was 133 (35–556) days. The radiation dose was 0.65 mSv (0.40–1.32 mSv). Assessment of the anastomotic site was excellent with the intra-observer agreement (κ) of 1.000, and inter-observer agreement (κ) of 0.889. Nine patients had the central type and the remaining 9 with the lateral type.
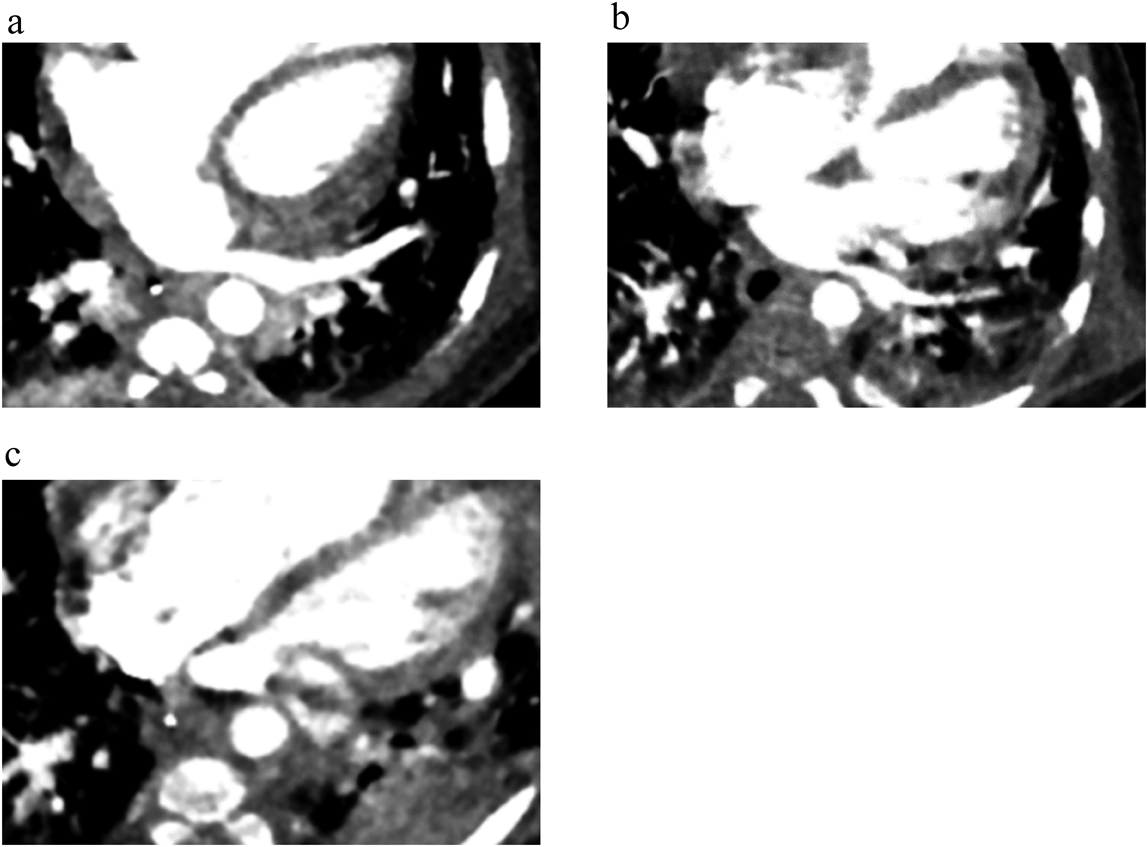
On CT, the PV was found flattened or stenosed in 9 patients (5 with the central type and 4 with the lateral type, p=0.58). Of these, two exhibited a significant PVO waveform with a continuous flow pattern on echocardiogram, whereas pulmonary congestion was not obvious on echocardiogram or chest X-ray in the remaining 7. Eventually, 4 patients underwent reoperation due to postoperative PVO (1 patient with the central type and 3 patients with the lateral type, p=0.24). Two of them were patients with a continuous PV waveform on echocardiogram, and reoperated soon after CT imaging. In the other 2 patients, reoperation was postponed initially. Although PVO was suspected on CT imaging exhibiting stenosis with mild intimal hyperplasia, the blood flow pattern was not typical for PVO on echocardiography. The pattern was similar to that in other unreoperated patients with PV stenosis indicated by CT imaging. Further close observation, nonetheless, made us recognize symptoms of respiratory distress and feeding inability, which propelled us to reoperate them. For these two patients, we were unable to detect alteration of the blood flow pattern in the periodical follow up, presumably because PV stenosis was localized and blood flow across the responsible site had been decreased or even diminished. Subsequently, repeated assessment using contrast-enhanced CT indicated significant progression of PVO (Fig. 2). When comparing pre- and postoperative findings, the left PV became gradually flattened compressed by the descending aorta and the atrium, resulting in long segmental PVO. On the other hand, whether PVO developed or not was independent of location of the anastomotic site in this study (central type 1 in 5 patients, lateral type 3 in 4 patients, p=0.099).
Surgical outcomes of TAPVC repair have been improved11); still, the mortality rate remains high once postoperative PVO develops. Prevention and early detection of PVO play a significant role in the prognosis of TAPVC. While CT is a useful tool for the definitive diagnosis of TAPVC and PVO before any reparative procedure,12, 13) few studies have evaluated early detection of postoperative PVO of this modality. A concern for radiation-induced cancer has globally expanded efforts to reduce radiation exposure doses, particularly in the children.14–17) We retrospectively analyzed impact of CT imaging for early detection of postoperative PVO using 320-row MDCT.
The introduction of 320-row MDCT to our hospital enabled examination at a low radiation exposure dose, by which a single scan can cover a wide range of the heart; specifically, the equipment can scan the whole heart in a single heartbeat in small children.18) During the study period, contrast-enhanced CT was performed in patients with repaired TAPVC approximately 3 months after surgery, for the purpose of follow-up or early screening of PVO. Our study clearly indicated that 320-row MDCT was operated with a radiation exposure dose less than 1 mSv, which was lower than that of 64-row MDCT used in the previous study by Frush et al.15) Although the radiation exposure to the heart should be minimized to prevent subsequent heart failure or carcinogenesis,19) our result implied that the 320-row MDCT is acceptable as compared with previous CT devices, particularly when high spatial resolution of CT is essential for indicating re-intervention.
Among the 4 patients reoperated, postoperative PVO was suspected before conducting contrast-enhanced CT in 2 patients based on echocardiography and their physical findings. In the remaining 2, contrast-enhanced CT showed flattening of the peripheral PV and mild intimal hyperplasia, while echocardiogram and other examinations including chest X-ray did not suggest pulmonary congestion. Based on changes in pre- and postoperative CT imaging, it was obvious that the left PV had got mechanical obstruction gradually. The orientation of the anastomotic site did not turn out to be a risk for postoperative PVO in our study. These findings implies that CT imaging is capable of predicting progressive PVO with which physical findings would appear eventually. On the other hand, echocardiography should have been carried out more frequently to assess the PV in these cases; then, progressive PV stenosis could have been detected.
The evaluation of postoperative PVO approximately 3 months after surgery was considered reasonable, as Ricci et al. reported that postoperative PVO frequently occurred within 6 months after surgery in their echocardiographic study.20) The median period between the primary repair and the reoperation was less than a few months in our patients. This may imply that precise CT images are advantageous for early diagnosis of the stenotic PV requiring reintervention. Meanwhile, 5 out of 9 patients with PV stenosis on CT did not develop PVO or pulmonary congestion clinically; this represented low specificity of CT imaging in this respect. There is no room for doubt in high sensitivity of this modality when diagnosing PVO. Efforts to improve probability of the pretest should be implemented to minimize irradiation related with cardiac CT imaging even with 320-row MDCT. Accordingly, the appropriate timing of conducting advanced imaging techniques, including CT, needs to be clarified for early detection of postoperative PVO in the current era.
Limitations
The small number of patients assessed by CT hindered detailed analyses for patients` background, mechanisms of developing PVO and comparison with echocardiogram. Although current clinical practice and guideline for irradiation do not warrant additive radiation exposure, our study highlighted that use of objective imaging modality was important in the assessment of postoperative PVO. No alternative modality is available for 320-row MDCT in terms of spatial resolution at present, although examinations using advanced imaging technology without irradiation, such as cardiac MRI, could be combined to improve diagnostic accuracy of postoperative PVO.
Contrast-enhanced CT using 320-row MDCT takes place with a low radiation exposure dose, and could detect PVO in the peripheral region earlier than echocardiography did. In addition to stenosis at the anastomotic site, the positional relationships could be visualized around the spine, the descending aorta, and the peripheral PV in patients with postoperative PVO. Meticulous follow-up is recommended when CT demonstrates flattening of the PV and intimal hyperplasia, or when the initial TAPVC is classified as the lateral type.
謝辞Acknowledgments
The authors acknowledge Dr. Satoshi Nakano and Dr. Yurie Takizawa (Iwate Medical University Hospital) for supporting this study.
Financial Disclosure
None.
Conflicts of Interest
All authors have no conflict of interest to declare.
引用文献References
1) Karamlous T, Gurofsky R, Sukhni EA, et al: Factors associated with mortality and reoperation in 377 children with total anomalous pulmonary venous connection. Circulation 2007; 115: 1591–1598
2) Yong MS, d’Udekem Y, Robertson T, et al: Outcome of surgery for simple total anomalous venous drainage in neonates. Ann Thorac Surg 2011; 91: 1921–1927
3) Friesen CLH, Zurakowski D, Thiagarajan RR, et al: Total anomalous pulmonary venous connection: An analysis of current management strategies in a single institution. Ann Thorac Surg 2005; 79: 596–606, discussion, 596–606
4) Nakayama Y, Hiramatsu T, Iwata Y, et al: Surgical results for functional univentricular heart with total anomalous pulmonary venous connection over a 25-year experience. Ann Thorac Surg 2012; 93: 606–613
5) Kelle AM, Backer CL, Gossett JG, et al: Total anomalous pulmonary venous connection: Results of surgical repair of 100 patients at a single institution. J Thorac Cardiovasc Surg 2010; 139: 1387–1394
6) Jacobs JP, Anderson RH, Weinberg PM, et al: The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. Cardiol Young 2007; 17 Suppl 2: 1–28
7) Sugimoto K, Miyaji K, Oka N, et al: Conventional repair of total anomalous venous drainage without primary sutureless technique: Surgical tips to prevent pulmonary vein obstruction. Gen Thorac Cardiovasc Surg 2018; 66: 405–410
8) Honjo O, Atlin CR, Hamilton BC, et al: Primary sutureless repair for infants with mixed total anomalous pulmonary venous drainage. Ann Thorac Surg 2010; 90: 862–868
9) Craig JM, Darling RC, Rothney WB: Total anomalous pulmonary venous drainage into the right side of the heart: Report of 17 autopsied cases not associated with other major cardiovascular anomalies. Lab Invest 1957; 6: 44–64
10) Latson LA, Prieto LR: Congenital and acquired pulmonary vein stenosis. Circulation 2007; 115: 103–108
11) Kirshbom PM, Myung RJ, Gaynor JW, et al: Preoperative pulmonary venous obstruction affects long term outcome for survivors of total anomalous pulmonary venous connection repair. Ann Thorac Surg 2002; 74: 1616–1620
12) Oh KH, Choo KS, Lim SJ, et al: Multidetector CT evaluation of total anomalous pulmonary venous connections: Comparison with echocardiography. Pediatr Radiol 2009; 39: 950–954
13) Shen Q, Pa M, Hu X, et al: Role of plain radiography and CT angiography in the evaluation of obstructed total anomalous pulmonary venous connection. Pediatr Radiol 2013; 43: 827–835
14) Brenner D, Elliston C, Hall E, et al: Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol 2001; 176: 289–296
15) Frush DP, Yoshizumi T: Conventional and CT angiography in children: Dosimetry and dose comparisons. Pediatr Radiol 2006; 36 Suppl 2: 154–158
16) Vassileva J, Rehani MM, Applegate K, et al: IAEA survey of paediatric computed tomography practice in 40 countries in Asia, Europe, Latin America and Africa: Procedures and protocols. Eur Radiol 2013; 23: 623–631
17) Mousavi-Gazafroudi SS, Sajjadieh-Khajouei A, Moradi M, et al: Evaluation of image quality and radiation dose in low tube voltage coronary computed tomography angiography. ARYA Atheroscler 2019; 15: 205–210
18) Shirota G, Maeda E, Namiki Y, et al: Pediatric 320-row cardiac computed tomography using electrocardiogram-gated model-based full iterative reconstruction. Pediatr Radiol 2017; 47: 1463–1470
19) Saiki H, Moulay G, Guenzel AJ, et al: Experimental cardiac radiation exposure induces ventricular diastolic dysfunction with preserved ejection fraction. Am J Physiol Heart Circ Physiol 2017; 313: H392–H407
20) Ricci M, Elliott M, Cohen GA, et al: Management of pulmonary venous obstruction after correction of TAPVC: Risk factors for adverse outcome. Eur J Cardiothorac Surg 2003; 24: 28–36, discussion, 36
 ,Shin Takahashi,Takuya Takahashi,Hirofumi Saiki,Kotaro OyamaHiroshi Toyoshima
,Shin Takahashi,Takuya Takahashi,Hirofumi Saiki,Kotaro OyamaHiroshi Toyoshima