There have been reports of femoral arteriovenous fistulae due to trauma or acquired medical factors,1, 2) but no reports of congenital femoral arteriovenous fistulae have been found. Persistent left-to-right shunting caused by femoral arteriovenous fistulae increases preload and leads to high cardiac output heart failure.3, 4) We report a case of congenital left femoral arteriovenous fistula with symptoms of heart failure from the neonatal period. Written informed consent for publication was obtained from the parents.
The baby was born at a local obstetrics and gynecology clinic via vaginal delivery at 39 weeks and 6 days of gestation, with an Apgar score of 9/9 and birth weight of 3,046 g. No use of forceps or vacuum on delivery, and there was no trauma on her body. Distressed breathing appeared from postnatal Day 3, and the patient was transferred to the previous neonatal intensive care unit on Day 7. On echocardiography, the right atrium and right ventricle were enlarged, and the inferior vena cava (IVC) was dilated, indicating congestive heart failure. However, congenital heart disease was not detected, and oral diuretic therapy improved her symptoms. She was transferred to our hospital for further investigation and treatment on Day 18.
She was active and showed no clinical signs of heart failure. And she had never received any punctures at her both femoral areas. However, transthoracic echocardiography still showed IVC dilation (7.9 mm) and right ventricle volume overload. NT-proBNP levels were still elevated (10,266 pg/mL). While we were unable to detect the cause of heart failure, she recovered well and was discharged on Day 37 with diuretic treatment. The diuretic was discontinued at 53 days of age. After 15 days of diuretic interruption, her left thigh became swollen (Fig. 1) and she had to be re-hospitalized. Her vital signs were as follows: weight 5,400 g, heart rate 122/min, blood pressure 89/61 mmHg, respiratory rate 42/min, and SpO2 100% (room air). Lower extremity findings were a left thigh circumference of 23.5 cm, right thigh circumference of 21.0 cm, left lower leg systolic pressure of 70 mmHg, right lower leg systolic pressure of 72 mmHg, palpable thrill at the left inguinal region, and an audible Levine 4/6 continuous murmur. Chest radiography showed cardiomegaly (cardiothoracic ratio (CTR) 60%). Transthoracic echocardiography showed right atrium and right ventricle volume overload, but no valvular diseases nor congenital heart diseases. The cardiac index was estimated to be 8.6 L/min/m2.
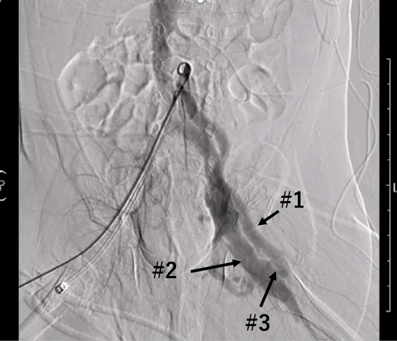
Lower extremity angiography was performed, which revealed a shunt from the left femoral artery to the left femoral vein. The SaO2 of the superior vena cava (SVC) was 62.6%, while the IVC was high at 94.1% (Fig. 2). We diagnosed a left femoral arteriovenous fistula and high cardiac output heart failure and performed arteriovenous fistula ligation on 78 days of life.
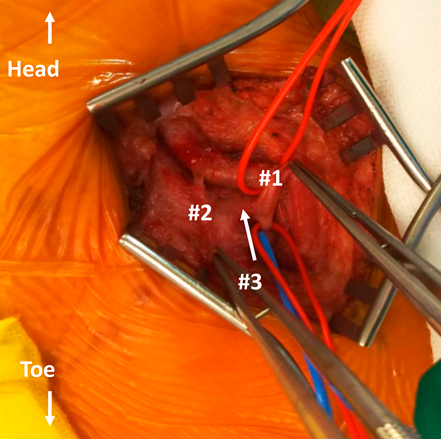
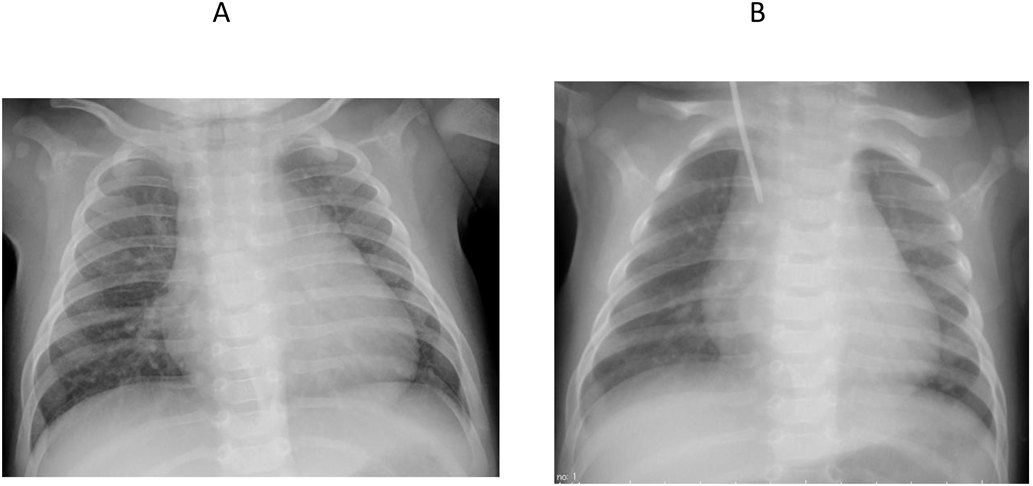
On the operation, a fistula from the superficial femoral artery to the superficial femoral vein was found, and a double ligation was performed (Fig. 3). The patient’s clinical symptoms and NT-proBNP levels improved immediately after the surgery (1,804 pg/mL), and cardiothoracic ratio on chest radiography improved (Fig. 4). She was discharged from the hospital on 84 days of life. She has been well without any symptoms and arteriovenous shunt including recurrence of left femoral fistula has not been observed.
Acquired femoral arteriovenous fistulae have been reported to be traumatic or medically induced, and there have been reports of patients developing heart failure.3, 4) In adult patients, there are reports of bilateral femoral arteriovenous fistulae5) and cases of Kasabach-Merritt syndrome,6) but we could not find any reports in neonates without a history of trauma or a possible medical origin. Regarding for congenital disorders, Parkes Weber syndrome (PWS) and hereditary hemorrhagic telangiectasis (HHT) are known for causing arteriovenous fistula. PWS is a congenital vascular malformation and high output cardiac failure is reported in 31% of cases. High output cardiac failure is usually due to large arteriovenous malformation and anemia, which can be sometimes fatal in pediatric patient.7) On the other hand, HHT is multiple organ disease characterized by repeated bleeding of skin, mucosa and intestine. Atrio-venous malformation of brain, spine, lung and liver are noted.8) However, both PWS and HHT usually show skin lesions suggesting micro-vascular anomalies, which our patient did not have. Also, our patient did not have skeletal or soft tissue anomalies nor any signs of bleeding. We concluded the possibility for congenital disorders were quite rare. Furthermore, collagen diseases may have been associated with congenital arteriovenous fistula, but we did not find any signs suggesting collagen diseases.
Heart failure caused by a femoral arteriovenous fistula is high output heart failure with symptoms of body congestion from excessive preload. In previous reports, the symptoms of heart failure appeared at 8 months9) or 14 years3) after the formation of the arteriovenous fistula; in this case, the symptoms appeared at an extremely early age of 3 days, which suggested that the patient was already in a high cardiac output state before delivery. Shibuya10) pointed out that the causes of high cardiac output heart failure in the fetal period can be divided into arteriovenous shunts and peripheral vasodilation. In this case, there was no evidence of fetal edema, which may indicate severe heart failure, and the heart failure worsened after birth due to an arteriovenous shunt. This may be because the placenta, which has low vascular resistance, is in equilibrium with the systemic vascular resistance during the fetal period, and peripheral circulation can be maintained, making heart failure less likely to occur.11) However, due to the increase in systemic vascular resistance after birth, arteriovenous shunt flow tends to increase, leading to high cardiac output heart failure.
 1,Ryuji Fukazawa1,Makoto Watanabe1,Kanae Tsuno1,Masanori Abe1,Kenji Suzuki2,Takashi Sasaki2,Yosuke Ishii2,Yasuhiko Itoh1Ryosuke Matsui
1,Ryuji Fukazawa1,Makoto Watanabe1,Kanae Tsuno1,Masanori Abe1,Kenji Suzuki2,Takashi Sasaki2,Yosuke Ishii2,Yasuhiko Itoh1Ryosuke Matsui