The patient was a 6-year-old boy who had previously been well, except for allergic rhinitis caused by mite and house dust. He had no history or family history of KD. During class one morning, he experienced acute chest pain in the precordial area and vomited. He appeared ill, pale and lethargic, and was taken to the emergency room at our hospital. On admission, he was afebrile and his vital signs indicated HR 77 beats/min, BP 90/64 mmHg, RR 24 breaths/min, and SpO2 97% on ambient air. He was asleep, but awakened appropriately upon examination. All other physical findings were normal.
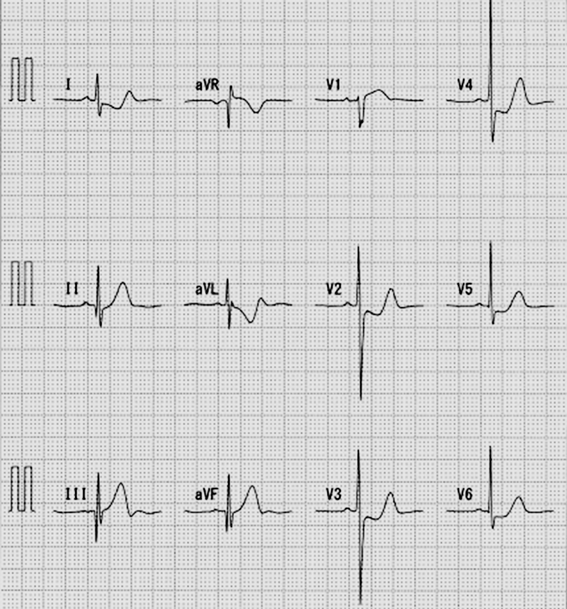
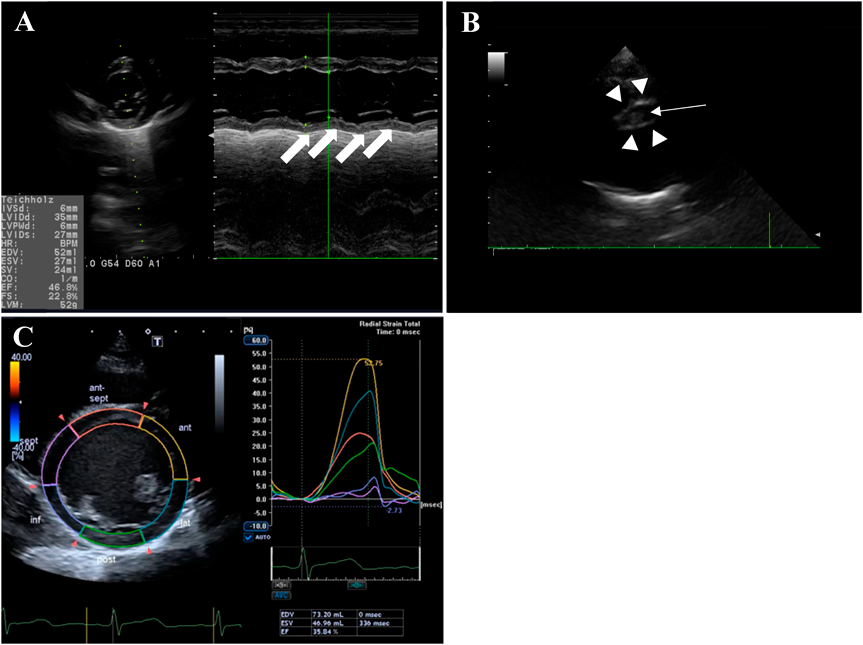
Electrocardiography (ECG) showed sinus rhythm with deep Q in III and aVF, ST elevation in I and V1, and ST depression in V2–V6 (Fig. 1). Echocardiography revealed impairment of the left ventricle (LV), with LV ejection fraction (LVEF) of 46.8% (Fig. 2A). The patient was admitted to the PICU on suspicion of acute myocarditis, and 3 µg/kg/min dobutamine and 0.5 µg/kg/min milrinone were started. Laboratory data were: WBC: 12.900/µL; RBC: 443×104/µL; Hb: 12.5 g/dL; PLT: 29.8×104/µL. Renal function, electrolytes, and standard coagulation values were within normal limits. Serological markers of myocardial damage were unremarkable: GOT: 30 U/L; LDH: 248 U/L; CPK: 149 U/L; CK-MB: 23 U/L; TnT: 0.025 ng/mL; NT-pro BNP: 166 pg/mL; BNP: 20.7 pg/mL.
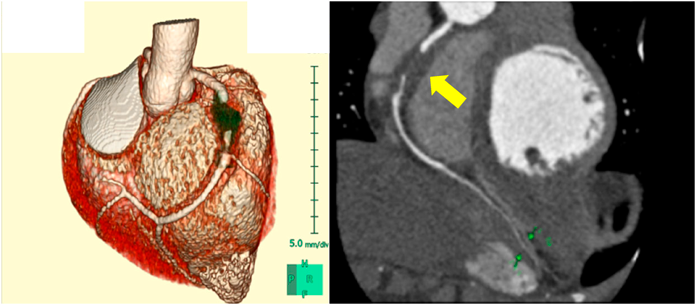
Re-echocardiography in the PICU revealed severe dilatation of the RCA (7.4 mm, Z+9.1) with a low echoic lesion suggesting thrombosis (Fig. 2B) and reduced wall motion in the inferior-posterior area of the LV (Fig. 2A). Echocardiography with two-dimensional speckle tracking (2DST) revealed low radial strain in the inferoseptal and inferior areas (Fig. 2C). Circumferential and longitudinal strain were also low in the same areas. Multi-low detector computed tomography (MDCT) showed occlusion of the RCA at the #2 segment due to thrombus formation with aneurysmatic dilatation of about 2.0 cm in length and 7.0 mm in diameter. The distal segments of the RCA (#3, #4) provided contrast (Fig. 3).
Based on these findings, the patient was diagnosed with AMI subsequent to thrombotic occlusion due to a right CA. Anticoagulation therapy with heparin and warfarin was started, combined with aspirin. Blood pressure, pulse and urine volume stabilized after starting dobutamine and milrinone. ACE inhibitors were started on day 4 of hospitalization and β-blockers were started in small doses on day 15. The heparin dose was adjusted to give an activated partial thromboplastin time between 50 and 70 s, and warfarin was adjusted to give an international normalized ratio of the prothrombin time of 2 to 3. The final doses were 0.1 mg/kg/day warfarin and 5 mg/kg/day aspirin. LVEF improved to ≥50% after the start of catecholamine and chest lead ST depression on the ECG also improved, but BNP remained high at 200 pg/mL. CK-MB (431 U/L) and troponin (7.5 ng/mL) peaked on the day after admission and declined thereafter.
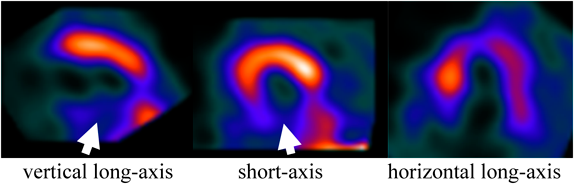
During hospitalization, the patient had no chest pain or symptoms such as fever, rash or arthritis, and no abnormal immunological markers or autoantibodies (C3: 142 mg/dL; C4: 39 mg/dL; CH50: 50.7 mg/mL; anti-nuclear antibody: <40 times; anti-DNA antibody: <2.0 IU/mL; anti-SS-A antibody: <1.0 U/mL; anti-SS-B antibody: <1.0 U/mL; antiglomerular basement membrane antibody: <2.0 IU/mL; proteinase-3-antineutrophil cytoplasmic antibody (ANCA): <1.0 U/mL; myeloperoxidase-ANCA: <1.0 U/mL). On day 20 after admission, resting myocardial scintigraphy (Tc-99 m tetrofosmin) showed decreased accumulation in the LV lower wall (Fig. 4). The patient was discharged on day 22.
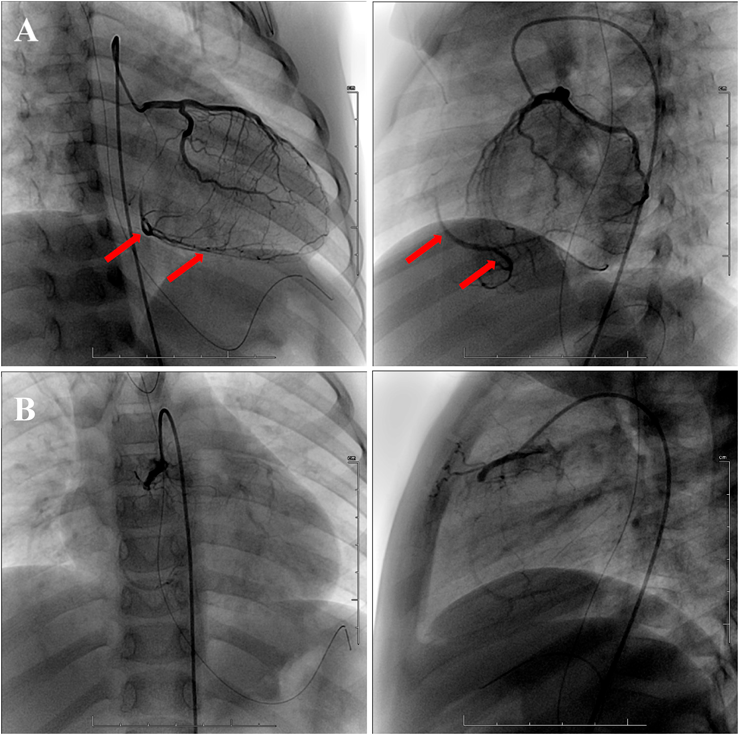
At three months after admission, left coronary angiography (CAG) showed no dilatation or stenosis through the left coronary artery (LCA) and supply to the RCA distal segment via a well-developed collateral circulation from the LCA (Fig. 5A). Right CAG revealed complete occlusion of the RCA with formation of a slight collateral circulation from the proximal RCA (Fig. 5B). The patient has been maintained with ACE inhibitors, β-blockers, warfarin, and aspirin, and has continued to undergo regular echocardiography and ECG as an outpatient. LVEF has improved to ≥60%. The abnormal Q wave of III and aVF remain on ECG, but ST of the chest leads has normalized.
Coronary aneurysms (CAs) are often asymptomatic, but can develop with angina, myocardial infarction, heart failure and sudden death. The frequency of coronary aneurysm on adult CAG is 0.15 to 4.9%, with a half being atherosclerotic lesions.2) Other causes include KD, Takayasu disease, conjunctive tissue disease (Marfan syndrome, Ehlers-Danlos syndrome), other forms of vasculitis (lupus, polyarteritis nodosa, Behcet’s disease, rheumatoid arthritis, ankylosing spondylitis, scleroderma), infections (human immunodeficiency virus, bacterial, mycobacterial, syphilis, lyme disease, mycotic aneurysm, septic emboli), drugs (cocaine, amphetamine, protease inhibitors), and chest trauma.3) In Japan, KD accounts for 15–20% of CAs4) and 5% of cases of acute coronary syndromes in patients under 40 years old are due to KD CAs.5)
It was unclear if the patient in our case had KD or incomplete KD before admission, but there was no history of fever, conjunctivitis or rash that suggested KD, including in infancy. At 1 and 4 months before admission, the patient had only one febrile episode for 1 to 2 days without other symptoms. Patients younger than 12 months with KD tend to have incomplete KD and are at risk of developing coronary aneurysms.6) These cases include a 12-week-old infant with fever and rash who developed multiple giant CAs,7) and a conference report of an infant who died suddenly after only one episode of fever and was found at autopsy to have a coronary aneurysm that pathologically resembled a KD CA.8) Another conference report described a pediatric case with no history of KD, in which old myocardial infarction was pointed out in school ECG and a CA was found by CAG.9)
In our case, differential diagnosis of the cause of CA was performed during hospitalization (some data not shown). Takayasu disease was excluded due to lack of findings of vascular stenosis on echo or contrast examination during catheterization. Conjunctive tissue disease, including Marfan syndrome, was ruled out based on physical examination and echocardiography. Other forms of vasculitis, including lupus, were excluded based on the absence of autoantibodies, and lack of characteristic findings and other diagnostic criteria. Drugs and trauma were ruled out based on medical history. There were no clear signs or laboratory data suggesting infection; thus, a detailed examination was not conducted, so this cause of onset of CA could not formally be excluded.
A comparative study of CA diameters in KD and febrile children suggested that a CA Z score >2.5 is specific to KD.10) Our case had a giant RCA aneurysm, which is likely to be a complication of KD, particularly since 40% of myocardial infarctions after KD are reported to develop within 3 months and 73% within 1 year.11) Thus, fever in our patient 1 month or 4 months before admission may have been due to KD, and an RCA giant aneurysm due to incomplete KD with fever merely may have developed.
In Japan, school ECG may be useful for early detection of CAs that may progress asymptomatically. In ECG examination of 17 children with KD myocardial infarction, deep and wide Q waves were often observed in anterior wall and septal side wall infarction. Six of 7 cases of inferior wall infarction showed deep Q waves, but only one case had a width ≥0.04 s.12) Our patient underwent a school ECG examination 4 months before admission, and deep Q in III was found, but the voltage was <0.5 mV. This range does not meet the secondary test criteria for school ECG. Exercise stress ECG might have assisted, but early detection could still have been difficult because the CA might have developed after ECG was performed.
There have been many reports of thrombolytic therapy using ulinastatin and t-PA during catheter interventions for occlusion due to CAs in KD, but there are few reports in patients with no history of KD.13) Our case had no history of KD, the causative disease was unknown, and the patient was stable, even after myocardial infarction. Thus, it was difficult to decide whether to use thrombolytic therapy due to concerns of serious side effects such as intracranial hemorrhage. Therefore, heparin and anti-heart failure treatment were used.
No abnormality was found in left CAG in our case, but an aneurysm at the left coronary artery may have regressed and normalized. However, future evaluation of the vascular lumen using intravascular ultrasound is needed to monitor possible progression of stenosis.
It is difficult to make a judgement of KD in febrile pediatric patients with three or fewer common manifestations of KD. Chest pain is a frequent complaint in children, and mostly noncardiac in origin. Myocardial ischemia or infarction in childhood is rare. However, regardless of the cause of myocardial infarction in children, management with acute treatment such as thrombolytic therapy and catheter treatment is necessary.
 1,Satoshi Onishi2,Yo Okizuka2,Hiroaki Minami1Takamichi Uchiyama
1,Satoshi Onishi2,Yo Okizuka2,Hiroaki Minami1Takamichi Uchiyama