Coronary artery fistula (CAF), defined as an abnormal connection between the coronary artery and a cardiac chamber, occurs in 0.3% of congenital heart disease.1) A fistula originates from the right coronary artery (RCA) (52%) or the left coronary artery (43%),2) and mainly terminates at the right side of the heart; the right ventricle (40%), the right atrium (25%), or the pulmonary artery (20%).3)
Surgery has been the first-line treatment for CAF. Some recent studies have also discussed transcatheter closure as an alternative procedure for management of CAF. We herein report a rare form of CAF from the RCA draining into the left ventricle (LV) in an infant, in whom the fistula was percutaneously closed using an Amplatzer™ Vascular Plug II (AVP II) (St. Jude Medical, Inc., Saint Paul, MN, USA) for the first time in Japan.
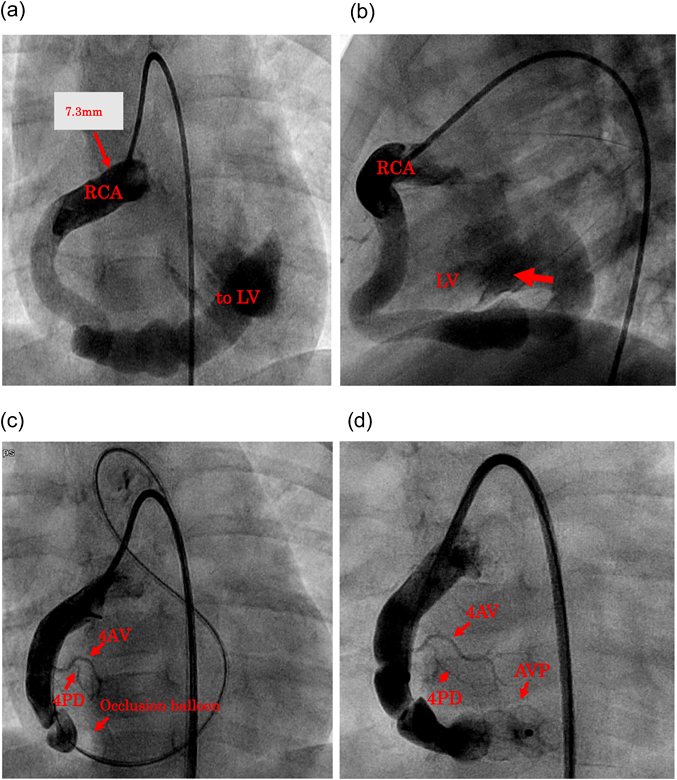
A female baby, born at 41 weeks and 1 day of gestation and weighing 2,832 g, was diagnosed with a RCA-LV fistula detected from a heart murmur after birth at a local hospital. She was treated with diuretics and antiplatelet agents at the hospital. No signs of heart failure or angina pectoris were noted in her clinical course. At 15 months old, cardiac catheterization and enhanced computed tomography (CT) were performed. On CT, the RCA was obviously dilated with a diameter of 7.3 mm, supplied perfusion to the myocardium normally, and had a connection to the area adjacent to the mitral valve in the LV (RCA-LV fistula). The diameter of the fistulous pathway ranged from 6 mm to 10 mm without localized stenosis. The orifice opening to the LV was 12.5 mm. The left coronary artery was normal. Cardiac angiography showed that the LV was markedly enlarged with an end-diastolic volume of 50 mL (239% of the anticipated normal value), indicating that the fistula should be closed.
The patient was referred to our hospital for the treatment at 21 months of age (body height 81.7 cm and weight 10.7 kg). Her vital signs were; pulse rate 98 beats/min, respiratory rate 24 breaths/min, blood pressure 98/50 mmHg, and SpO2 95% in room air. On auscultation, a Levine grade 1 diastolic murmur (mid-pitched) was heard at the right sternal border in the third intercostal space. We opted for catheter intervention because of its less invasive nature. Based on RCA angiography (Fig. 1a, b), we initially attempted to place coils into the CAF.
Firstly, we created a guidewire loop. From the right femoral artery (RFA), a 4 Fr Judkins right coronary catheter was inserted into the RCA. Through it, we advanced a microcatheter (Leonis Mova, Sumitomo Bakelite Co., Ltd., Tokyo, Japan) as well as a 0.018″ guidewire (Thruway, Boston Scientific, Marlborough, MA) to the RCA, the LV, the ascending aorta, and subsequently to the descending aorta. The tip of the guidewire was grasped with a 4 Fr 10-mm loop snare catheter (Amplatz gooseneck snare, Ev3 Inc., Plymouth, MN) advanced from the contralateral left femoral artery (LFA). Then, the tip was pulled out of the body through a sheath placed at the LFA, and the wire loop was secured in the sequence of RFA-RCA-LV-Aorta-LFA.
Secondly, a 4 Fr wedge pressure balloon catheter (Alpha Medical Instruments, LLC., CA, USA) was advanced from the LFA into the RCA over the wire loop. We repeated test balloon occlusion in order to identify an appropriate site for embolization without ST changes on electrocardiogram. RCA angiography illustrated the fistula distal to the posterior descending branch (4PD) (Fig. 1c) when the fistulous communication was test occluded. We decided to close the channel distally to the origins of the 4PD and the posterior atrioventricular branch (4AV), and paid attention to avoid protrusion of an occluder into the LV cavity. The maximum vessel diameter of the site was 6.8 mm. Use of coils did not appear appropriate, and we chose a 10-mm-diameter AVP II in the long and large segment.
A short sheath at the RFA was removed. We advanced a 5 Fr flexible guiding sheath (Flexor® Ansel Guiding Sheath No. 2, Cook Medical Japan G.K., Tokyo, Japan) anterogradely to the distal end of the embolization site. Then, an AVP II was deployed there. We repeated angiography through the guiding sheath to prove that the device was at the optimal embolization site (Fig. 1d). We detached the AVP II after confirming no ST changes noted on electrocardiogram, no obstruction of the branches of the normal coronary artery on repeated angiography, and no mitral regurgitation or stenosis on transthoracic echocardiography. Angiography after implantation showed only a small residual shunt. No complications occurred.
Antiplatelet (aspirin 5 mg/kg, per os) and anticoagulant drugs (warfarin 0.05 mg/kg, per os) were administered immediately after the procedure. Repeated transthoracic echocardiography showed no residual shunt. Pericardial effusion was noted and LV contraction slightly decreased. Therefore, we administered an oral diuretic (furosemide 1 mg/kg, per os) and a vasodilator (enalapril maleate 0.05 mg/kg, per os). The patient was discharged home 7 days after the intervention without increase of pericardial effusion. She was kept on the oral diuretic and the vasodilator. Pericardial effusion disappeared by follow-up 4 months time.
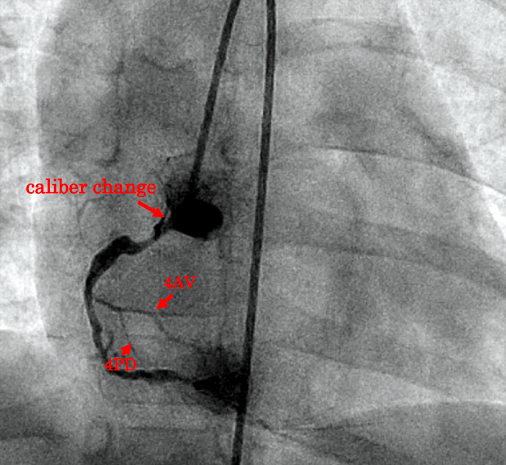
One year and 5 months after the intervention, the patient underwent RCA angiography to evaluate changes in the RCA following CAF closure. The proximal portion of the RCA was patent. There had been a caliber change there, with a vessel diameter of approximately 1.6 mm (Fig. 2). Therefore, antiplatelet agents and anticoagulants were continued.
CAFs are uncommon and have an estimated incidence of 0.002% in the general population.4) The RCA to LV fistula is even rarer, accounting for only 0.3% of all CAFs.5) Hemodynamically, the abnormal communication resembles aortic regurgitation and may cause heart failure due to volume overload to the LV or angina due to the so-called coronary steal phenomenon. On the other hand, some patients remain asymptomatic as was the case in our patient.
Konno et al.6) proposed the following criteria for the treatment of CAFs in adult patients: (asymptomatic with a shunt volume >30%, (2) presence of ischemic changes on electrocardiogram, (3) a history of infectious endocarditis, (4) progression of congestive heart failure expected, (5) a history of aneurysmal formation of the coronary artery posing a potential risk of rupture, and (6) causing a significant heart murmur and a social disadvantage. The indication and timing of treatment for an asymptomatic lesion is controversial because some CAFs close spontaneously.7) Our patient had a heart murmur, left ventricular volume overload, and no tendency to CAF regression. We judged that closure of the CAF was sensible.
Surgical closure has been the mainstream for treatment of CAFs. Nowadays, the efficacy of transcatheter approach has been reported in some cases. Catheter intervention for CAF was first reported in 1983 by Reidy et al. using a detachable balloon.8) Since then, various devices have been used, including coils,9) umbrella devices,9) a covered stent,9) and Amplatzer™ Duct Occluder (ADO, Abbott, Chicago, IL).10) In recent years, possibility of a residual shunt, mortality, and complications after transcatheter closure are shown to be equivalent to those after surgical closure.11)
This type of catheter intervention may require a time-consuming process before acquisition of the technique. Vascular dissection or thrombosis at the point of device detachment, and possible dislodgement of the material are other factors to realize.12) In contrast, the procedure is less invasive, a patient would experience a shorter recovery time, and the overall cost could be lower than that by surgery, because it does not require a midline sternal incision or artificial heart-lung device.13)
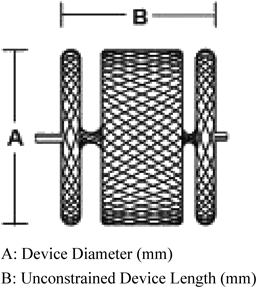
Use of the AVP II has attracted attention in recent years (Fig. 3). This device seems advantageous over other devices in three aspects. Firstly, large sizes of the product are available and allow sufficient closure of vessels, even large, without placing too many devices.12, 13) Secondly, the six-sided structure is expected to ensure reliable embolization, which may shorten procedural time and reduce costs.12) Thirdly, angiography is repeatedly feasible prior to detachment of the AVP II. This enables the operator to adjust the position of the device precisely in the vessel. The device can be readily visualized in relation to the normally formed coronary arterial branches and the orifice of the fistula to the cardiac chamber. Implantation of the AVP II is, accordingly, well-controlled and more secure compared with coils.12)
Furthermore, the caliber of the sheath used for the device can be smaller than that for other products of the Amplatzer™ family (e.g., ADO), making it possible to treat infants or small children.14) Taking these features into account, the AVP II is particularly suitable for closing large CAFs. Using this material, catheter intervention is considered as a reasonable alternative to surgical option. In our patient, we decided to choose catheter intervention, because we judged that her body size was large enough so that her CAF could be safely closed with the approach.
Regarding the device size of the AVPII, some reports recommended use of a device 175–200% of the minimum lumen diameter,15, 16) while others suggested that a 130–150% size would be justified even leaving a small residual shunt because such a minor communication should spontaneously close off.13, 17) In the present patient, the diameter of the shunting vessel was as large as 6.8 mm. We selected a 10-mm-diameter AVP II, rather than coils, the size being approximately 150% of the vessel diameter. The device turned out to be reliable for securely closing her giant fistula as expected. As for the approach, we opted for a prograde maneuver through the RCA. A retrograde approach through the orifice in the LV was considered difficult in this 10 kg infant in terms of angulation of the catheter pathway.
Coronary arterial obstruction is known to be a sequela after surgical closure of CAF. Anticoagulation including use of antiplatelets should be necessary even after similar treatments by catheter intervention. Routine coronary angiography is also pertinent after the treatment to evaluate patency and the circumstance of the coronary arteries.
There is a risk of thrombus formation in a dilated coronary artery; shear stress onto the vascular wall had been increased because of a high-velocity and a large amount of blood flow through the vessel, and damages to the intima could have been induced prior to interventional treatment. Once a CAF is occluded, blood flow becomes stagnant, and the dilated coronary artery carries a high risk of thrombosis. Anticoagulation therapy is necessary for an extended period of time after CAF closure.18)
Additionally, the affected coronary artery could become slender, stenotic or even occluded over time after CAF closure. Such obstruction, although complete occlusion is rare, may not present obvious ischemic symptoms, because the contralateral coronary arterial system could supply blood flow to the myocardium of the affected area.19) Even if a patient is asymptomatic, periodic coronary angiography and myocardial scintigraphy are considered essential to clarify whether any clinically significant stenosis is present across the affected coronary arterial pathway. In our patient, it was found obvious that the caliber at the RCA origin had changed on coronary angiography within one year after CAF closure. We decided to continue antiplatelet and anticoagulant therapy, since narrowing might develop still further eventually. As for pericardial effusion and a mild decrease in LV contraction seen after the procedure, we considered that inflammatory response to the device placed was the pathophysiological cause. Aspirin, a diuretic, and a vasodilator orally administered were effective, providing rapid improvement in these phenomena.
We report successful transcatheter closure of a large CAF using a 10 mm-sized AVP II in an infant, which was the first case in Japan. This procedure was safe, reliable, less invasive and, at the same time, cost-effective. We regard this approach as an alternative to surgical closure of CAFs.
Informed Consent
Informed consent was obtained from the parents of the patient. This report was conducted in accordance with the Declaration of Helsinki.
Funding
The authors have no funding sources relevant to this article to disclose.
Financial Disclosure
The authors have no financial interests relevant to this article to disclose.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Originally published in Journal of JPIC, Vol. 4 (2019), pp. 6–10. [in Japanese]
引用文献References
1) McNamara JJ, Gross RE: Congenital coronary artery fistula. Surgery 1969; 65: 59–69
2) Levin DC, Fellows KE, Abrams HL: Hemodynamically significant primary anomalies of the coronary arteries angiographic aspects. Circulation 1978; 58: 25–34
3) Lowe JE, Oldham HN Jr., Sabiston DC Jr.: Surgical management of congenital coronary artery fistulas. Ann Surg 1981; 194: 373–380
4) Luo L, Kebede S, Wu S, et al: Coronary artery fistulae. Am J Med Sci 2006; 332: 79–84
5) Zheng J, Dong R, Liu T, et al: Giant right coronary artery aneurysm with a fistula to the left ventricle. Ann Thorac Surg 2012; 94: 149–150
6) Konno S, Endo M: Congenital coronary artery disease. Kokyu To Junkan 1973; 21: 397–409 (in Japanese)
7) Reidy JF, Sowton E, Ross DN: Transcatheter occlusion of coronary to bronchial anastomosis by detachable balloon combined with coronary angioplasty at same procedure. Br Heart J 1983; 49: 284–287
8) Perry SB, Rome J, Keane JF, et al: Transcatheter closure of coronary artery fistulas. J Am Coll Cardiol 1992; 20: 205–209
9) Mullasari AS, Umesan CV, Kumar KJ: Transcatheter closure of coronary artery to pulmonary artery fistula using covered stents. Heart 2002; 87: 60
10) Al-Ata J, Amin M, Galal MO, et al: Transcatheter occlusion of a large left coronary artery to right superior vena cava fistula using the Amplatzer duct occlude device. Pediatr Cardiol 2004; 25: 70–72
11) Armsby LR, Keane JF, Sherwood MC, et al: Management of coronary artery fistulae: Patient selection and results of transcatheter closure. J Am Coll Cardiol 2002; 39: 1026–1032
12) Yadav A, Buxi TB, Jayamma SS, et al: Coronary cameral fistula treated by the Amplatzer vascular plug. Jpn J Radiol 2014; 32: 608–612
13) Liang CD, Ko SF, Lin YJ, et al: Transcatheter closure of a left circumflex coronary artery fistula in two children using the Amplatzer vascular plug. Pediatr Cardiol 2009; 30: 1172–1175
14) Wiegand G, Sieverding L, Kaulitz R, et al: Transarterial and transvenous approach for transcatheter closure of a large coronary artery fistula with the Amplatzer vascular plug. Pediatr Cardiol 2009; 30: 172–175
15) Fischer G, Apostolopoulou SC, Rammos S, et al: Transcatheter closure of coronary arterial fistulas using the new Amplatzer vascular plug. Cardiol Young 2007; 17: 283–287
16) Kassaian SE, Alidoosti M, Sadeghian H, et al: Transcatheter closure of a coronary fistula with an Amplatzer vascular plug: Should a retrograde approach be standard? Tex Heart Inst J 2008; 35: 58–61
17) Balaguru D, Joseph A, Kimmelstiel C: Occlusion of a large coronary-cameral fistula using the Amplatzer vascular plug in a 2-year old. Catheter Cardiovasc Interv 2006; 67: 942–946
18) Matsuura H, Kato M, Hoshida H, et al: Congenital RCA-LV fistula with unexpected finding in post-operative coronary angiography: A case report. Heart 1999; 31: 735–740
19) Momma K, Takao A, Imai Y: Coronary arteriovenous fistula with aneurysm which was obstructed with thrombus after surgery. Heart 1988; 20: 727–732
 ,Yoshitsugu Nogimori,Kazuhisa Sato,Yosuke Kitagawa,Takuya Wakamiya,Shin Ono,Ki-Song Kim,Sadamitsu Yanagi,Hideaki UedaAkio Kato
,Yoshitsugu Nogimori,Kazuhisa Sato,Yosuke Kitagawa,Takuya Wakamiya,Shin Ono,Ki-Song Kim,Sadamitsu Yanagi,Hideaki UedaAkio Kato