A female infant with no prenatal diagnosis was born to a healthy mother at 39 weeks’ gestation with a birthweight of 2,230 g at a previous hospital. Soon after birth, severe aortic stenosis and mitral regurgitation were diagnosed. Percutaneous balloon aortic valvuloplasty (PTAV) at ages 1 and 2 months relieved the symptoms temporarily, but restenosis soon developed. She was transferred to our hospital for further evaluation at age 3 months.
On admission, her general appearance was fair; her body weight was 4,584 g, with body height 50 cm. Her blood pressure was 83/67 mmHg, pulse 160/min, and respiratory rate 33/min with an O2 saturation of 100% under oxygen administration 0.5 L/min. A cardiac murmur was detected at the second intercostal space at the left sternal border with Levine 3/6 blooming and at the fourth intercostal space with Levine 2/6 rumbling.
Laboratory test findings were unremarkable except for brain natriuretic peptide 1,455 pg/mL. The preoperative electrocardiogram showed deep Q wave at II, III, aVf, V5, V6, which implied severe LV hypertrophy. Echocardiography revealed an aortic valve annulus size of 6.9 mm (89% of normal, Z=−1.5) The right coronary cusp had been fused with the non-coronary cusp. The left coronary cusp was hypoplastic, and adherent to the non-coronary cusp at their commissures. Subendocardial myocardium appeared brighter than normal, being suggestive of myocardial ischemia. Doppler echocardiography illustrated peak jet velocity through the aortic valve to be 3.8 m/s, corresponding to pressure gradient (PG) 58 mmHg (mean: PG 33 mmHg) and an effective orifice area index of 0.39 by 3-dimensional planimetry. The LV was severely dilated, with the LV end-diastolic dimension 159% of the normal value. Ejection fraction was 37% with severe mitral regurgitation. These findings indicated that the patient was suffering from afterload mismatch. Other parameters, such as diastolic transmitral flow velocity or isovolumic relaxation time, were not suggestive of diastolic dysfunction. Because the patient had already received PTAV twice at the previous hospital, surgical repair of the aortic valve was planned within a few days.
The surgeon performed a commissurotomy and repaired the hypoplastic cusps with the patient’s own pericardium. Initially, mitral regurgitation was thought to be functional and was expected to recover quickly without intervention. Even after reduction of the LV load on cardiopulmonary bypass, however, mitral regurgitation failed to improve, prompting us to concomitant mitral valvuloplasty.
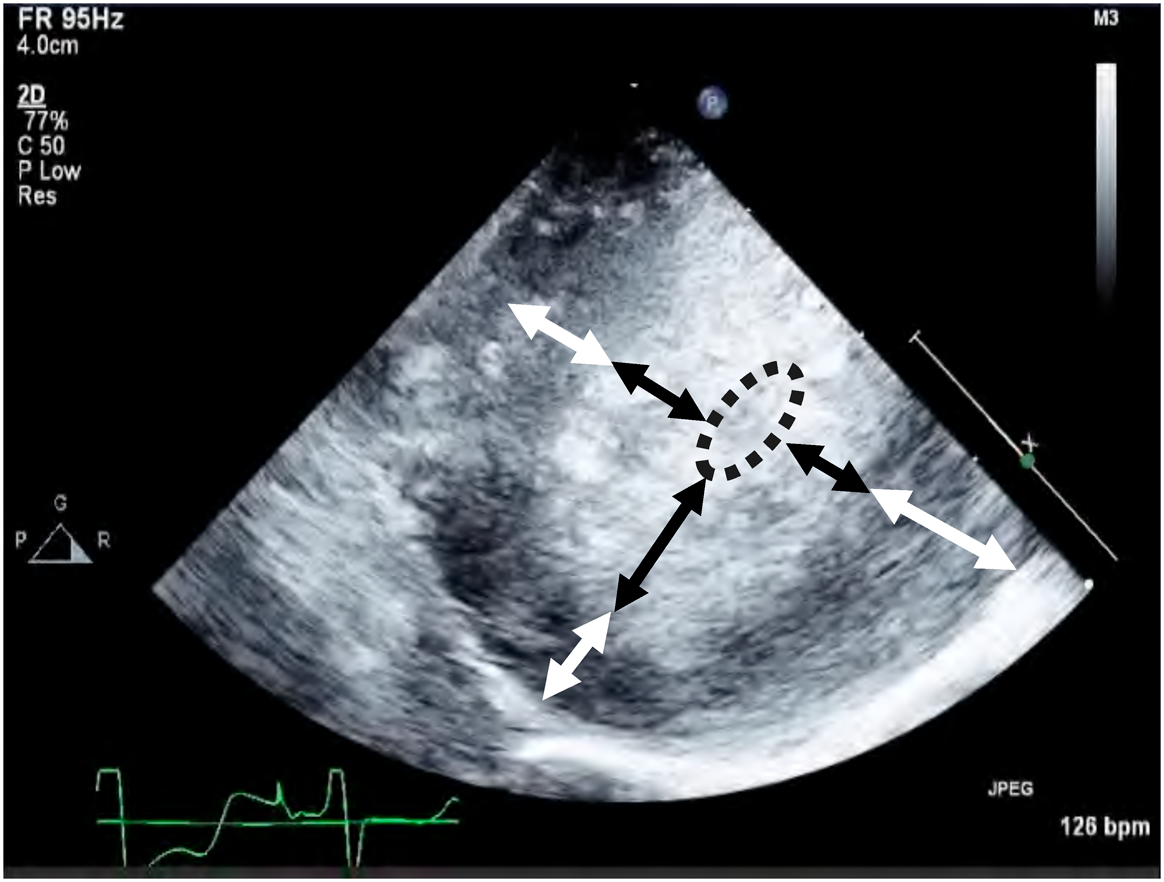
Intracardiac repair was completed within 136 minutes of cardiac arrest. Off cardiopulmonary bypass was attempted but infeasible. Blood pressure could not be maintained even with a large amount of inotropic support and additional volume infusion. After these interventions, epicardial echocardiography showed severely thickened LV wall and a nearly empty intraventricular cavity during attempted weaning from cardiopulmonary bypass (Fig. 1), probably due to adverse effect of long aortic cross-clamp time. No LV output was observed, and the aortic valve was non-functional. The patient was therefore placed on ECMO.
Cardiopulmonary bypass was switched to ECMO, a 10-Fr aortic cannula was placed in the ascending aorta, and a 14-Fr venous cannula was placed in the right atrium. For additional LV venting, a 14-Fr cannula was placed from the LV apex to decompress the left side of the heart and prevent development of pulmonary venous congestion due to severely impaired LV function.
On her return to the cardiac intensive care unit (CICU), the patient stayed on ECMO at a flow rate of 300 mL/min (2.8 L/min/m2). Her mean systemic blood pressure was about 50–60 mmHg. Although there was no antegrade cardiac output under full ECMO support, the LV vent drained blood efficiently from the LV preventing LV dilatation and pulmonary venous congestion.
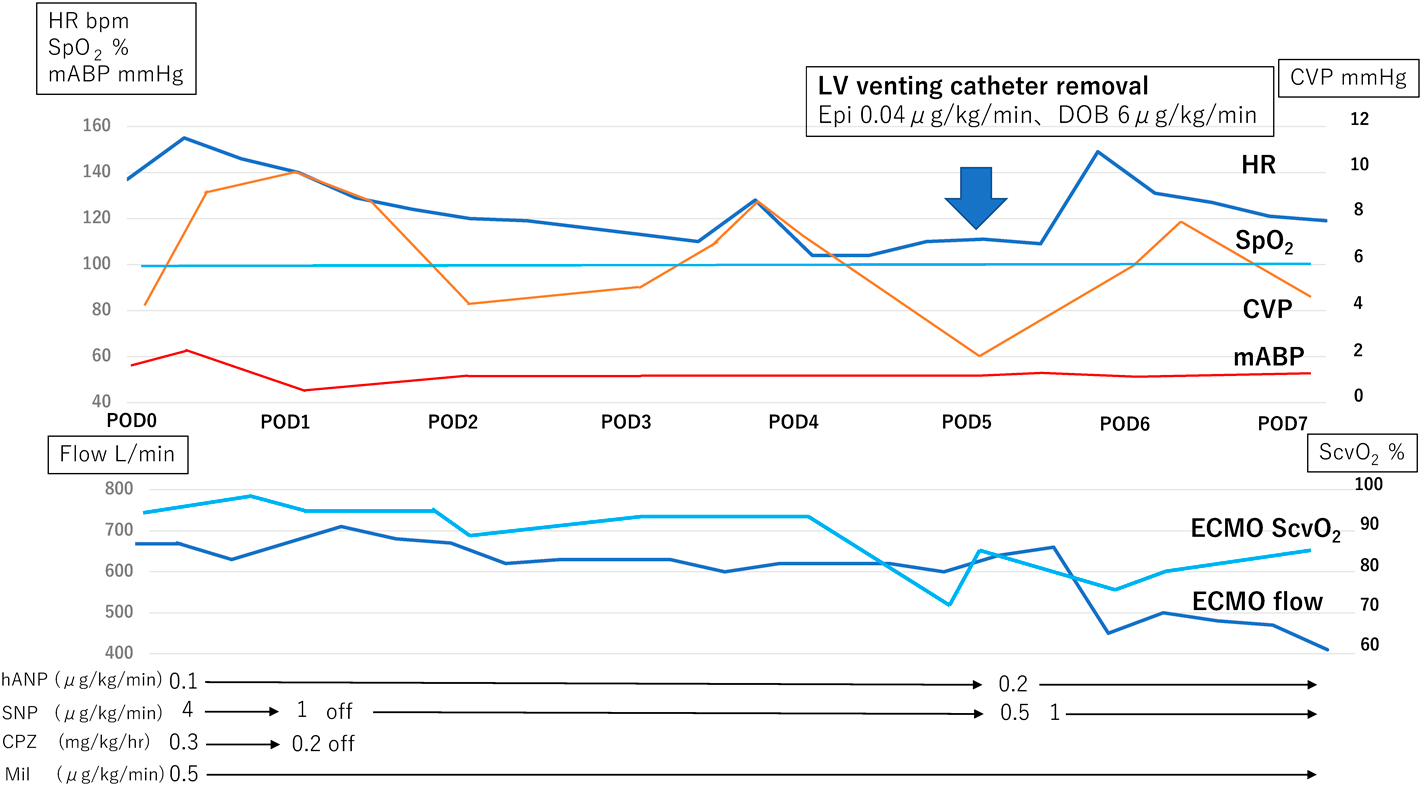
Her cardiac function gradually improved, and ejection across the aortic valve increased, enabling removal of the LV venting catheter on postoperative day 5 with central venous pressure 11 mmHg (Fig. 2). After catheter removal, the patient was able to maintain her LV output, with no deterioration of pulmonary congestion or mitral regurgitation. As native cardiac output increased, residual aortic valve stenosis and supra-valvar stenosis became unmasked which were of significant degrees. Surgical treatment was planned for those stenoses before weaning off ECMO. The surgeon found adhesion between the repaired aortic cusps which interfered with opening of the valve. Additionally, the suture lines from the previous operation had caused obstruction in the ascending aorta. After these residual lesions were revised, the patient was weaned off cardiopulmonary bypass without incident.
Unfortunately, she returned to the CICU on ECMO again for intraoperative airway bleeding, which subsided the following day. She was finally weaned off ECMO two days later. Her post-ECMO course was uncomplicated, and she was transferred back to the previous hospital without any neurological sequelae.
There are several mechanisms of LV dilation.1) (1) increased afterload induced by VA-ECMO in cases of LV failure; (2) suboptimal venous return accompanying right heart recovery; (3) heavy collateral bronchial flow; and (4) aortic insufficiency.
Even a small burden can be harmful in LV myocardial failure and lead to LV distention.
Zampi et al. reported that delays decompression of the left atrium (LA) or the LV were associated with longer duration of ECMO support and mechanical ventilation.2) Regardless of its cause, LV dilation should be avoided to promote the chances of myocardial recovery and to reduce the risk of pulmonary venous congestion. If pharmacological treatment is ineffective, surgical or catheter intervention should be considered.
The left side of the heart can be decompressed in various ways. An interatrial communication can be created at the bedside by catheter intervention.3) Although this procedure is less invasive than some others, it is not always successful because a thick atrial septum would be difficult to perforate A backup surgical procedure is therefore essential. Another possible issue is LV distension. This procedure decompresses only the LA. No matter how the LV fails, the structure still tries to suck blood from the LA and usually remains distended. This interferes with myocardial recovery. Furthermore, once LA decompression was successful, a thrombus might be formed in the LV. The interatrial communication created would need to be closed after the patient was weaned off ECMO.
Swartz et al. reported a successful case of LA cannula implantation, in which a sheath was inserted through the femoral vein and placed in the right atrium, then a cannula was advanced into the LA by puncturing the atrial septum under transesophageal echocardiography.4) Although a cannula in the LA decreases LA pressure efficiently, the possibility of LV distention and clot formation remain.
Use of Impella® is reportedly an effective method of decreasing LV distention associated with VA-ECMO.5) Impella® continuously drains the LV and delivers the blood to the proximal aorta, thus maintaining flow from the LV to the aorta even in the absence of LV ejection or opening of the aortic valve. Impella® can therefore be a viable option in children with a large body size. The risks of vessel trauma and various other events must be weighed against the benefits before use. In particular, use of Impella® combined with ECMO is associated with a higher risk of bleeding complications than Impella alone.
From the hemodynamic point-of-view, direct LV decompression is ideal and can be achieved most effectively via a cannula from the LV apex regardless of the amount of blood leaving the LA. Blood is drained through the LV cannula during either diastole or systole, resulting in much lower LV pressure than achieved by LA venting. Also, the blood circulates throughout the cardiac cycle in the severely dysfunctioning LV. This significantly reduces the risk of thrombosis. Still, meticulous care is required to avoid potential complications such as surgical bleeding and myocardial injury. In our case, we encountered no significant surgical bleeding, and could manage to maintain activated clotting time over 200 seconds, which was longer than our standard to control thrombotic tendencies.
In the present patient, the LV wall was unusually thick, and the LV output was insufficient at the time of attempted weaning from cardiopulmonary bypass. The LV cavity was extremely small. The residual LV outflow tract obstruction, which initially remained unnoticed, was probably an additional unfavorable factor. Even continuously on ECMO, the potential of pulmonary venous congestion and LV distention would have been a matter of concern unless the left was vented.
The decision was made to introduce a LV vent intraoperatively in favor of reliable decompression at once, rather than adding venting later. By venting the LV and decreasing LV diastolic pressure, LV distention and pulmonary congestion did not occur. This seemed to us a key issue to manage such a difficult case successfully.
In VA-ECMO, decompressing the left-side of the heart in a timely manner according to the patient’s hemodynamics sounds essential. A few case reports previously mentioned preferable use of LA/LV decompression supported by ECMO in pediatric patients. None of these, nonetheless, clearly demonstrated indication or efficacy of the maneuver. Indication, timing, and practical methods of left heart decompression need to be established.