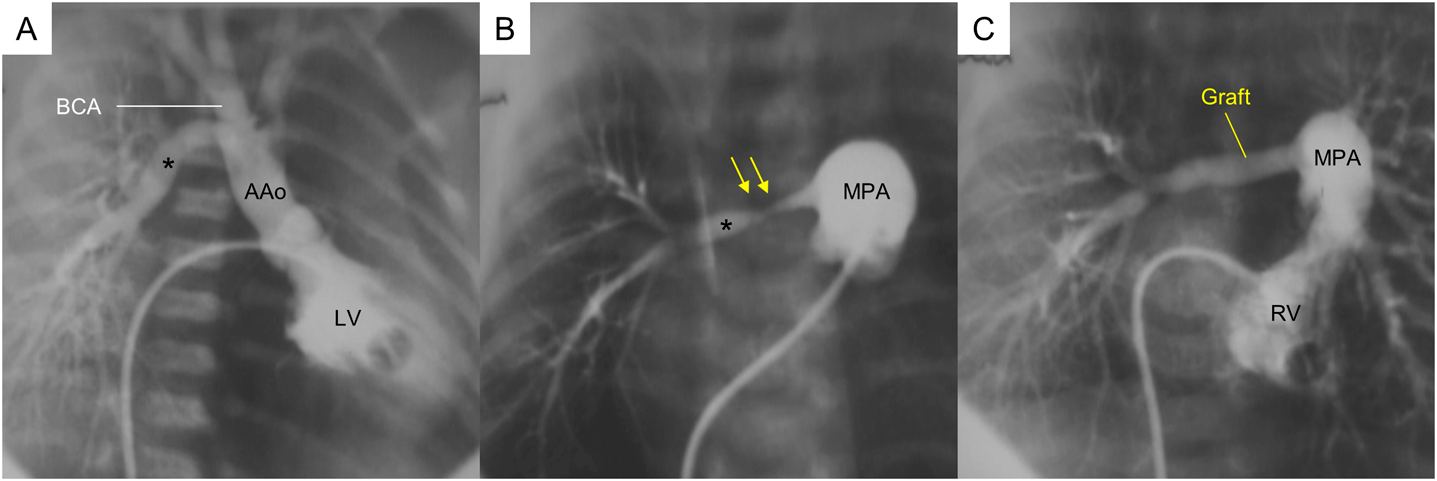
Anomalous Origin of the Right Pulmonary Artery from the Ascending Aorta with Aortic Coarctation
1 Department of Cardiovascular Surgery, JCHO Kyushu Hospital ◇ Fukuoka, Japan
2 Department of Pediatric Cardiology, JCHO Kyushu Hospital ◇ Fukuoka, Japan
受付日:2021年12月22日Received: December 22, 2021
受理日:2022年2月15日Accepted: February 15, 2022
発行日:2022年7月1日Published: July 1, 2022