The 3-year-old boy had been diagnosed as ARFID with food allergy to milk, eggs and wheat. At 2 years old, he was admitted to a hospital because of poor weight gain. He had mental retardation and eating disorders. The diagnosis of ARFID was made at that time. His diet was uneven, although he was able to eat white rice, salmon flakes, ham and spinach, and drink apple juice and tea. One month before admission this time, he could only eat white rice and tofu due to a mouth ulcer.
On admission, he was sluggish, and barely ate. Body weight was 10.3 kg (−2.1 SD) and height 86 cm (−2.5 SD). He presented no fever. Heart rate 160 bpm, respiratory rate 60/minute, blood pressure 78/40 mmHg, and SpO2 92% on ambient air. The patient appeared to be dehydrated with dry lips and a pale face. His mental status was as seen before. Physical examinations revealed an increased second heart sound, grade II systolic murmur at the left sternal border of the 3rd intercostal space, and retractive breathing. The liver was palpable one finger below the right costal margin. No edema was detected. Tendon reflex was weak in both upper and lower limbs. Blood tests showed an elevated lactate level and metabolic acidosis. Respiratory compensation had normalized pH. Inflammatory markers and liver enzymes remained low. No electrolyte imbalance was noted. Renal function was mildly impaired. NT-pro BNP was significantly elevated. Coagulation dysfunction was not obvious (Table 1).
Table 1 Laboratory data on admission| <BG(vein)> | <Biochemical and Endocrine> |
| pH | 7.387 | TP | 6.1 g/dL |
| pO2 | 45.7 mmHg | Alb | 4.0 g/dL |
| pCO2 | 23.0 mmHg | GOT | 35 U/L |
| HCO3− | 13.5 mmol/L | GPT | 28 U/L |
| BE | −9.8 | LDH | 520 U/L |
| Lactate | 30 mg/dL | CPK | 128 U/L |
| | T-Bil | 1.4 mg/dL |
| <CBC> | BUN | 19.7 mg/dL |
| WBC | 9,500/µL | Cr | 0.46 mg/dL |
| Hb | 10.5 g/dL | UA | 8.2 mg/dL |
| PLT | 17.5×104/µL | Na | 134 mEq/L |
| | K | 4.5 mEq/L |
| <Coagulation> | Cl | 103 mEq/L |
| PT-INR | 1.44 | Ca | 9.1 mg/dL |
| APTT | 29.1 sec | Glu | 117 mg/dL |
| Fib | 199 mg/dL | CRP | 0.09 mg/dL |
| D-dimer | 1.4 µg/mL | TSH | 1.55 µlU/mL |
| | fT4 | 1.05 ng/dL |
| | NTpro BNP | 35,000 pg/mL |
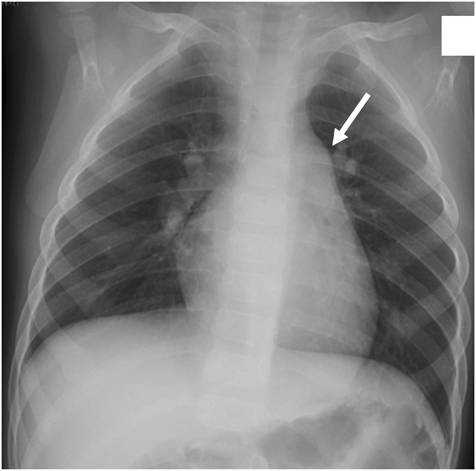
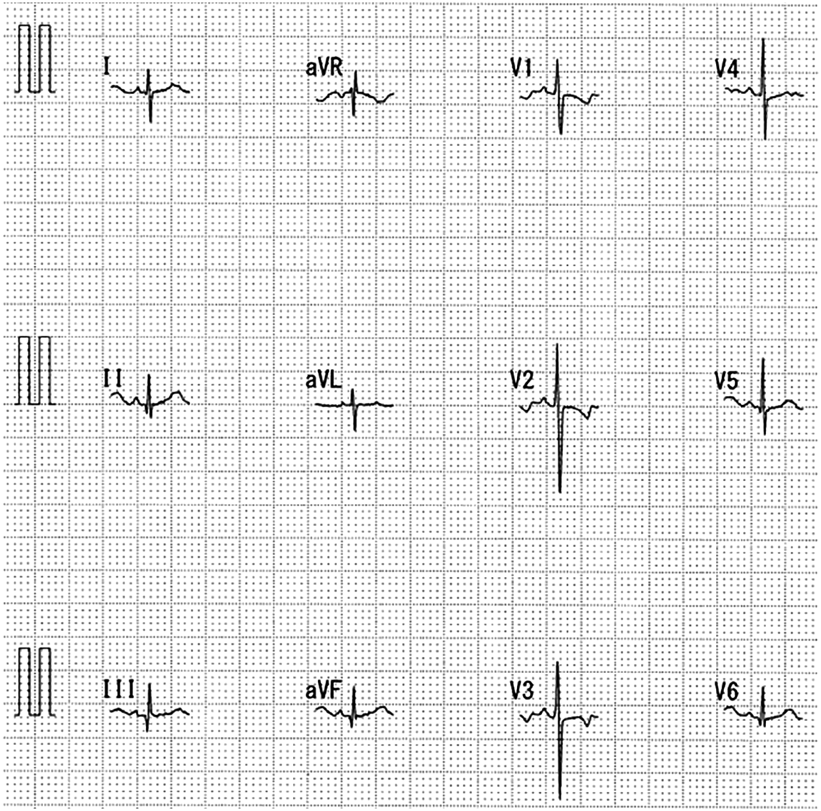
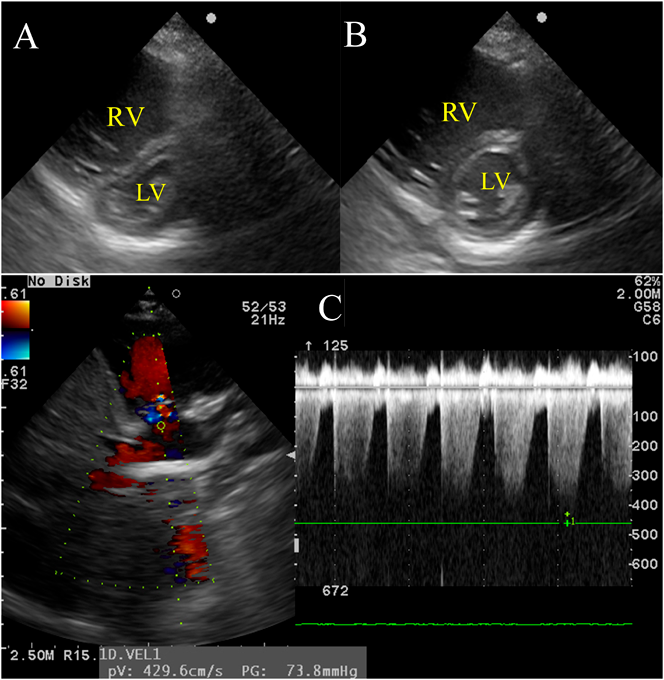
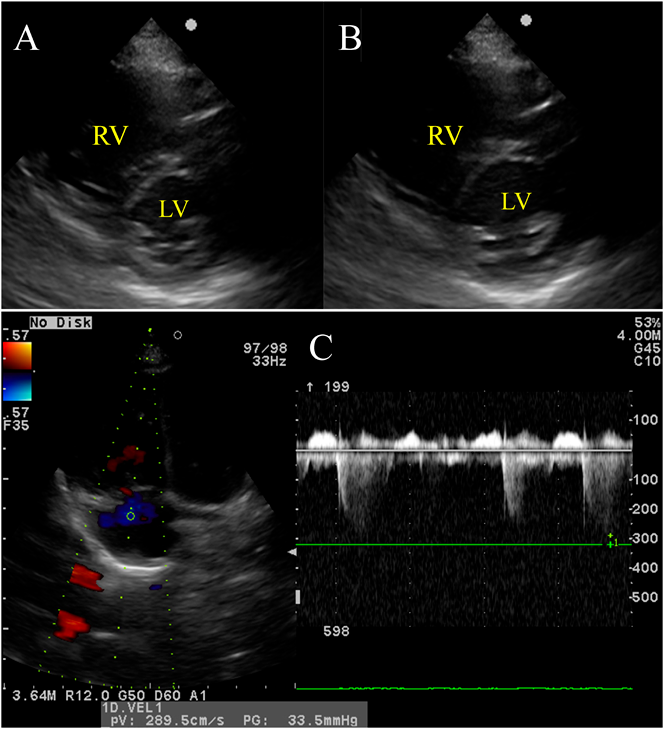
Chest radiography showed no abnormalities in the lung field and no cardiac enlargement. The main pulmonary artery was slightly enlarged (Fig. 1). Electrocardiography (ECG) showed a sinus rhythm with right axis deviation (Fig. 2). Echocardiography revealed enlargement of the right ventricle (RV) and right atrium (RA) and bulging of the interventricular septum to the left ventricle (LV). Tricuspid regurgitation (TR) was moderate, with a peak TR jet velocity of 4.29 m/s (Fig. 3). RV pressure was estimated to be 73 mmHg plus RA pressure; accordingly, severe PAH was suspected. Contrast echocardiography was performed to differentiate diseases causing hypoxemia. Microbubbles were stagnant in the RA and RV, with RV function markedly deteriorated, and did not enter into the left heart. A sildenafil (1 mg/kg) administration test was carried out through a nasogastric tube under oxygen administration using a high flow nasal cannula. One hour later, echocardiography showed that the abnormal arrangement of the interventricular septum had become normally round, that TR had improved to mild, and that the peak TR jet velocity had attenuated to 2.89 m/s (Fig. 4). Tachycardia and tachypnea disappeared, and blood pressure came up. Based on his dietary history, thiamine (30 mg) was injected intravenously followed by oral thiamine (25 mg/day) continued for possible cardiovascular beriberi due to vitamin B1 deficiency. Since idiopathic PAH could not be ruled out entirely, tadalafil (1 mg/kg/day) was started from the day of admission. TR eventually disappeared on echocardiography on the same day. The RV and the RA gradually became smaller.
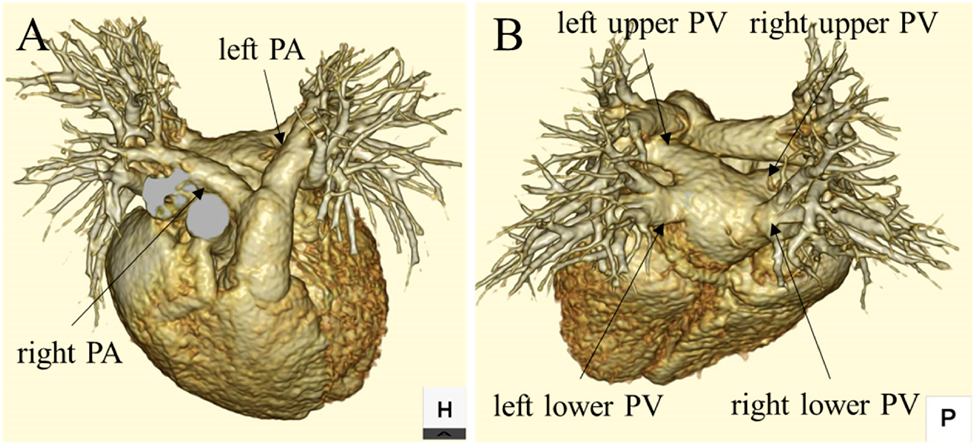
It turned out later that the vitamin B1 level on admission was 16 ng/mL (normal range: 20–50 ng/mL), suggesting vitamin B1 deficiency as suspected. In order to clarify the cause of PAH, contrast-enhanced CT was carried out. The pulmonary veins and arteries were normal. No filling defect was identified; pulmonary embolism was unlikely (Fig. 5). No abnormalities were noted in immunological markers and autoantibodies (C3: 64 mg/dL; C4: 31 mg/dL; CH50: 34.7 mg/mL; anti-nuclear antibody: <40 times; anti-DNA antibody: <2.0 IU/mL; anti-SS-A antibody: <1.0 U/mL; anti-SS-B antibody: <1.0 U/mL). After commencement of treatment, oral intake increased and his unbalanced diet improved. The patient was discharged on day 19, with tadalafil continued. Since PAH due to beriberi associated with vitamin B1 deficiency was considered most probable and the possibility of idiopathic PAH was low, tadalafil was reduced and eventually discontinued at 7 months after the onset of the current episode; vitamin B1 was continued. Catheter examination at 8 months after the event showed no significant abnormalities: mean pulmonary artery pressure (PAP) 22 mmHg and pulmonary resistance (Rp) 3.17 Units/m2 (Table 2).
Table 2 Data from cardiac catheterization| RAp | 7 mmHg |
| RVp | 32/6 mmHg |
| PAp | 30/12/22 mmHg |
| PA wedge p | 10 mmHg |
| LVp | 70/10 mmHg |
| Cl | 3.8 L/min/m2 |
| Rs | 10.85 Wood units×m2 |
| Rp | 3.17 Wood units×m2 |
| CI: cardiac index, Rs: systemic resistance |
Vitamin B1 deficiency resulting in cardiovascular beriberi has been reported as a cause of reversible PAH, although this has become a rare disease in Japan in recent years.1) Pediatric case reports of vitamin B1 deficiency associated with PAH have primarily involved long-term soft drink overconsumption, an unbalanced diet, or eating disorder due to mental retardation.2–4)
Vitamin B1 acts as a coenzyme in the process from glycolysis to the citric acid cycle, in which pyruvic acid is decarboxylated to produce acetyl-CoA. In case vitamin B1 is deficient, pyruvate is not oxidized and accumulates in blood and tissues, which increases lactic acid in blood and dilates peripheral blood vessels due to a decrease in peripheral vascular resistance. Fluid retention due to vasodilation results in activation of the renin-angiotensin-aldosterone system, leading to high output heart failure. Increases in pulmonary blood flow and pulmonary artery wedge pressure due to increased end-diastolic pressure in the LV lead to pulmonary venous hypertension.5) The mechanism of PAH in vitamin B1 deficiency has been speculated to involve direct impairment of myocardial energy production as well. Biventricular dysfunction can occur in deficiency of this substance; the RV is more profoundly affected than the LV. Lactic acidosis, once occur, can cause acute pulmonary vasoconstriction. Superoxide and reactive oxygen species produced by oxidative stress associated with vitamin B1 deficiency inactivate nitric oxide (NO), producing peroxynitrite as a powerful vasoconstrictor that can exacerbate PAH.6)
Our patient had suffered from ARFID. This condition can be due to avoidant and restrictive eating related to fear of consequences (such as choking, vomiting, and nausea), sensory issues (related to smell, taste, and texture), and low appetite or disinterest in food. ARFID is also associated with comorbid neurocognitive conditions: particularly autism spectrum, anxiety, and attention-deficit/hyperactivity disorders.7) Oral intake in our patient often decreased when he caught a cold. The trigger of his current eating disorder was an oral lesion. The patient seemed prone to vitamin deficiency because food intake had been restricted for allergies to wheat, eggs, and milk. Until one month before admission, he could eat salmon flakes (rich in vitamin D and vitamin B12) and ham (rich in vitamin B1). White rice and tofu also contain vitamin B1, but its content is low. That is probably why vitamin B1 intake became insufficient by eating only white rice and tofu for a month prior to hospitalization.
Vitamins C, A, E, K and folic acid are involved in the NO metabolic pathway and may affect the pathophysiology of PAH.3, 8) Our patient drank apple juice before admission; that makes deficient vitamin C unlikely. Tofu contains large amounts of vitamins E and K, and a blood test showed no coagulation disorder. Food containing vitamin A and folic acid could not be ingested; there was a potential of deficiency of these substances. There were, nonetheless, no associated findings, such as skin disorders or anemia. We could have investigated these vitamins, but just checking vitamin B1 appeared enough. As a result, PAH improved without administrating vitamins other than thiamine. The cause of PAH was most likely deficient vitamin B1.
Cardiovascular beriberi is rare, whereas respiratory symptoms are noticeable. Patients are often treated, therefore, for an attack of bronchial asthma or infection of the lower respiratory tract in hospital before precise diagnosis.3, 4) As respiratory disorder and hypoxemia progress, ventilator management is performed, sedative hypotension is promoted, and catecholamines are administered. The pathophysiological condition of cardiovascular beriberi is high output heart failure due to decreased peripheral vascular resistance, and the circumstance would get worse by using vasodilatory drugs such as dobutamine.4, 9) Diuretics may exacerbate the condition by promoting urinary excretion of vitamin B1.4) In our case, PAH appeared to be of an idiopathic cause; estimated as high resistance and low output on echocardiography. There was no sign of high output heart failure on admission. Despite low blood pressure, respiratory control was judged possible using nasal high flow. Invasive treatment, such as tracheal intubation, was avoided through initial administration of sildenafil.
Sildenafil and tadalafil are PDE-5 inhibitors and major pulmonary vasodilators. NO has a vasodilatory effect, through activating guanylate cyclase in the vascular smooth muscle and producing cyclic guanosine monophosphate (cGMP). PDE-5 specifically hydrolyzes cGMP, and accordingly its inhibitors suppress degradation of cGMP, enhance NO signaling, and dilate the vascular smooth muscle. Thus, a PDE-5 inhibitor has a similar effect to that of NO inhalation therapy.10) When PAH is associated with cardiovascular beriberi, however, the pathophysiological condition may not be resolved by NO inhalation therapy, but be only improved after administration of thiamine.2) In our patient, administrated sildenafil improved PAH even before giving thiamine echocardiographically and alleviated symptoms. Sildenafil may be superior to NO inhalation therapy because the agent suppresses expression of PDE-5 in the RV myocardium contributing to improved RV function, and also increases cardiac output without elevating pulmonary capillary wedge pressure.11, 12) This aspect is important because the pathophysiology of cardiovascular beriberi is seemingly related to functional deterioration of both ventricles (especially the RV) in addition to pulmonary vasoconstriction.6) In this way, sildenafil improved PAH and RV function resulting in an increase in blood pressure, a decrease in heart rate and improvement of dyspnea in our case. Accumulating more cases of PAH due to cardiovascular beriberi, we would be able to identify which is more effective in these patients, NO inhalation therapy or sildenafil. At the same time, it is essential to supply vitamins as soon as possible when suspected to be deficient.
Catheterization was performed 8 months after the admission event; tadalafil had been reduced and discontinued. Mean PAP and Rp was slightly elevated (Table 2). Probably, chronic vitamin B1 deficiency prior to admission had already promoted pulmonary arterial remodeling. It is necessary to follow up whether PAH would re-exacerbate or improve on echocardiography. Nutritional management should be another issue to be continued.
In conclusion, a potential of PAH due to cardiovascular beriberi should be kept in mind if the physical condition deteriorates in a child with an eating disorder or unbalanced diet. Timely assessment using echocardiography, treatments according to appropriate understanding of pathophysiology, and supplementation of vitamin B1 are of particular importance in such cases.
 1,Kazuhiro Yamamoto2,Satoshi Onishi2,Yo Okizuka2,Atsuko Takei1,Hirotaka Minami1Saki Otao1, Takamichi Uchiyama
1,Kazuhiro Yamamoto2,Satoshi Onishi2,Yo Okizuka2,Atsuko Takei1,Hirotaka Minami1Saki Otao1, Takamichi Uchiyama