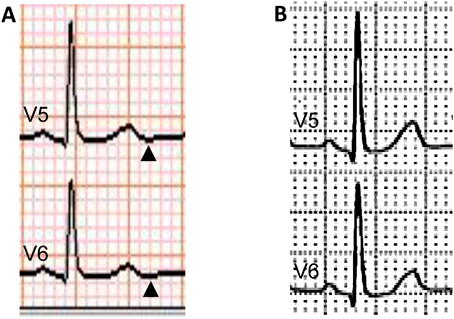
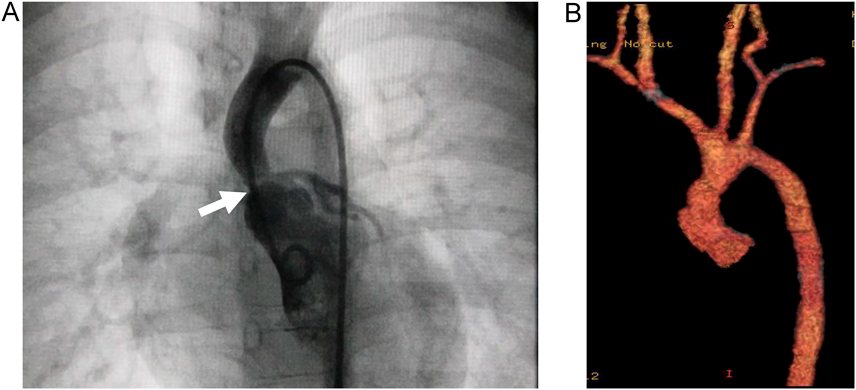
Negative U-Wave in Williams Syndrome with Supravalvar Aortic Stenosis
Department of Pediatrics, Hirosaki General Medical Center ◇ Aomori, Japan
受付日:2022年3月15日Received: March 15, 2022
受理日:2022年6月13日Accepted: June 13, 2022
発行日:2023年3月31日Published: March 31, 2023