Patient 1
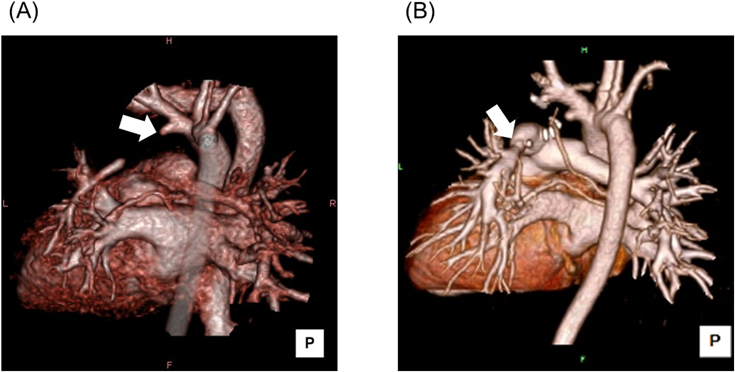
A 2-month-old female (weight 5.0 kg) with right aortic arch, left IPADO, and patent foramen ovale, was referred to our center for surgical treatment. Her diagnosis was confirmed by enhanced chest computed tomography and cine angiography, which revealed a diminishing ductus arteriosus from the brachiocephalic artery to the distal left PA which was hypoplastic (Fig. 1A). Imaging results raised concerns about a non-negligible difference in diameters and pulmonary vascular resistances between the right and left PAs. This could result in imbalanced PA flow after primary repair leading to non-symmetric PA growth, and, in particular, persistent hypoplasia of the left PA. Thus, we chose a staged approach. When over-shunted either by constructing a modified Blalock–Taussig (BT) shunt or stenting the duct, pneumorrhagia may be the result because of too much flow to the left PA, which may cause. On the other hand, if the initial shunt was too small, repeated construction of a shunt would be required with a short interal, because a 2-month-old baby could grow rapidly. Hence, we chose an original BT shunt, which becomes larger as the patient grows, for the first stage palliation. The original BT shunt was performed on the left side, followed by balloon angioplasty 3 months later.
At 11 months of age, catheterization confirmed the growth of the left PA, from 2.7 mm to 8.9 mm in diameter. The mean pressures of the right and left PAs were 23 mmHg and 22 mmHg, respectively.
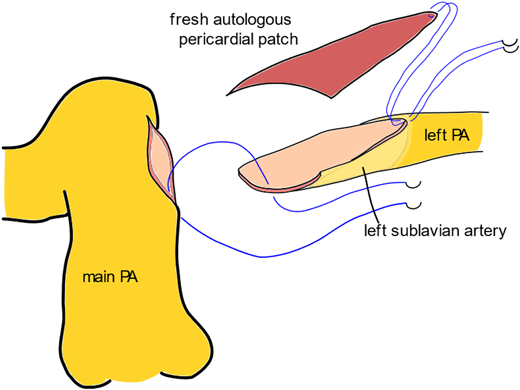
The patient underwent definitive repair at 14 months of age via a median full sternotomy on cardiopulmonary bypass with a beating-heart technique. The left PA seemed too distant from the main PA for a direct anastomosis. To interpose and reconstruct the posterior wall, a flap of the main PA or the left subclavian artery could have been used. We decided to choose the latter, because the previous site of the shunt anastomosis was distal, and use of the tissue as a flap was sensible to make the reconstruction certain. The left subclavian artery was divided at its origin and longitudinally incised. The incision was extended to the distal left PA across the previous anastomotic site, and augmented with a fresh autologous pericardial patch (Fig. 2). Finally, the reconstructed left PA was anastomosed to the left upper aspect of the main PA.
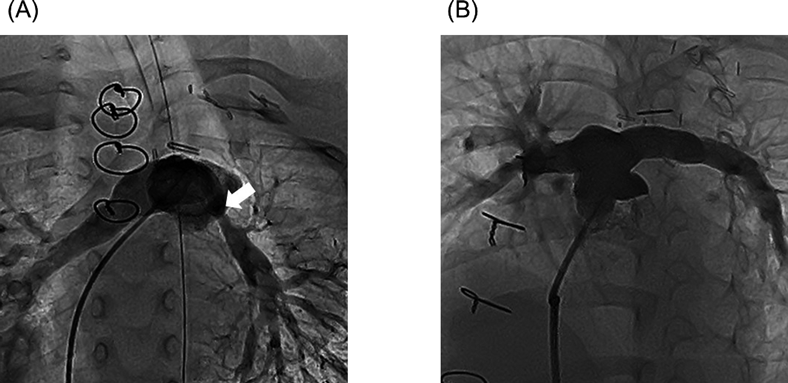
One month later, the mean PA pressure was 23 mmHg. Balloon angioplasty was performed for mild stenosis of the reconstructed left PA, and the stenotic region was dilated from 2.8 mm to 6.0 mm (Fig. 1B, Fig. 3A). The right-to-left lung perfusion ratio improved during follow-up from 3.63 at 2 months to 2.05 at 19 months after the definitive repair. Mean PA pressure and pulmonary vascular resistance also improved from 23 mmHg and 1.71 U·m2 at 1 month to 16 mmHg and 1.17 U·m2 at 13 months, respectively. The diameters of the bilateral PAs became more symmetrical (Fig. 3B). That of the right PA and the left PA were 7.3 mm and 7.6 mm, respectively. Pressure gradients between the main PA and the bilateral PAs also became equivalent: 9 mmHg for the right PA and 7 mmHg for the left PA at 13 months.
Patient 2
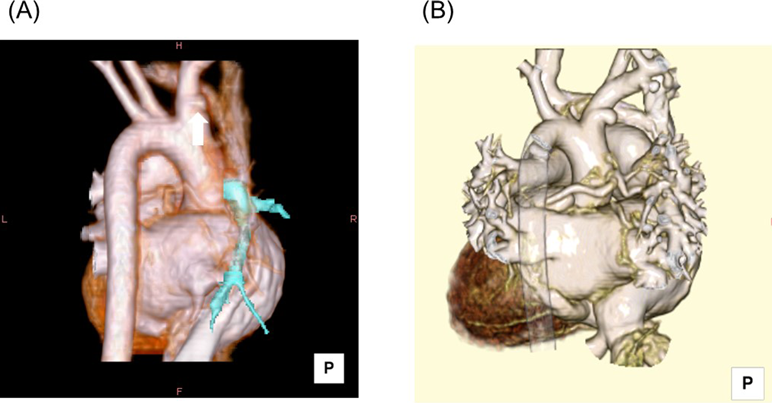
A 19-day-old male (weight 3.0 kg) with respiratory distress was referred to our center because his right PA was not detected on echocardiography. Right IPADO and a closed duct were confirmed by enhanced chest computed tomography (Fig. 4A). A modified BT shunt was constructed on the right side with a 3 mm expanded polytetrafluoroethylene tube as the first palliation. His native right subclavian artery did not seem suitable for directly anastomosing to the right PA as is the case with an original BT shunt procedure.
At 5 months of age, catheterization confirmed the growth of the right PA, from 2.2 mm to 7.5 mm in diameter. Mean pressures of the right and the left PAs were 7 mmHg and 27 mmHg, respectively.
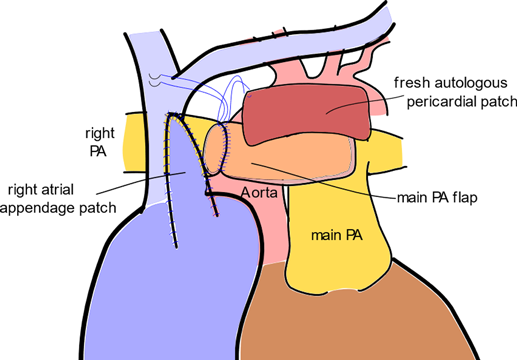
The patient underwent the definitive repair at 6 months of age (weight 8.0 kg) via a full median sternotomy on cardiopulmonary bypass with the heart beating. The previously placed shunt was removed, and the distal right PA was fully mobilized. Still, the distal right PA did not reach directly to the main PA. Therefore, a pedicled flap of the main PA was created, then anastomosed to the posterior aspect of the right PA; the route coursing in front of the ascending aorta in the form of a ‘unilateral’ Lecompte maneuver. If the route had been placed behind, we would have been worried about compression by the aorta onto the right PA, especially around the origin of the right PA (Fig. 5). The anterior wall of the right PA was augmented with a fresh autologous pericardial patch. The reconstructed right PA turned out to compress the superior vena cava (SVC), causing stenosis. Direct pressure measurement revealed pressure gradient of 5 mmHg between high SVC and the right atrium. Thus, we opened the proximal SVC longitudinally and covered the incision with the right atrial appendage, which decreased the pressure gradient.
One month later, enhanced chest computed tomography showed no stenosis (Fig. 4B). The right-to-left lung perfusion ratio was 1.14. Echocardiography 15 months after the definitive repair showed symmetric PA growth and blood flow distribution: the diameters of the right and the left PAs were 8.2 mm and 8.6 mm, and peak velocities (pressure gradients) were 1.2 m/s (6 mmHg) and 1.3 m/s (7 mmHg), respectively. Because of this favorable outcome, this patient has not been catheterized postoperatively.
The goal of surgical treatment for IPADO is to create a double-PA system from the main PA, providing balanced distribution of blood flow. It is essential to equalize vascular resistance in both lungs and to encourage to develop the vascular bed of the affected side before surgically incorporating the PAs. Also, it is important to maintain the growth potential of the reconstructed PA in order to avoid late reoperation for stenosis or occlusion.
While primary repair is described as advantageous to establish physiologically normal pulmonary circulation at an early stage and to reduce the number of surgeries, it is accompanied with frequent re-interventions, including PA stenting.3–5) Regarding growth of the reconstructed PA and blood flow distribution to that side, outcomes in the literature vary across studies.6, 7) Batlivala et al. reported that primary repair promoted growth of the affected PA effectively and improved distribution of blood flow.6) In contrast, a multi-center study by Goldstein et al. found that staged repair yielded better improvement in the z-score of the PA size and more balanced PA blood flow distribution when adjusted for group characteristics.7) Because the affected PA was already hypoplastic in either of our present patients, staged repair was to be justified.
When the affected PA is contralateral to the aortic arch, it usually originates from the duct at the base of the brachiocephalic artery.8) In such a circumstance, direct anastomosis to the main PA is unfeasible because the affected PA is remote from the main PA. In our first patient, the subclavian artery was initially used as a channel of the original BT shunt, and eventually contributed to reconstruction by extending the length of the distal left PA and connecting it to the main PA. In Patient 2, the wall of the main PA was utilized as a pedicled flap. Using these techniques, we can expect continuing natural growth of the reconstructed PAs, that should not be the case with an interposition method using various synthetic materials.5)
In summary, we have reported two surgical experiences of IPADO. Staged repair provided balanced distribution of blood flow to the bilateral lungs. The affected PA could be reconstructed with autologous vascular tissues, instead of prosthetic materials, promising potential of lifetime natural growth.
 ,Takaya Hoashi
,Takaya Hoashi