Aortopulmonary (AP) window is a communication between the main pulmonary artery (PA) and the ascending aorta (AscAo) in the presence of two separate semilunar valves. Mori et al.1) classified this rare subtype of congenital septal defect into three types; type I is a proximal defect located just above the sinus of Valsalva, type II a distal defect at the upper portion of the AscAo, whilst type III a large defect involving the majority of the AscAo, the mian PA and the right PA. AP window is extremely rare, accounting for 0.1–0.6% of congenital cardiac malformations. Though it may occur as an isolated lesion, it is more likely associated with other cardiac lesions.2, 3) These include atrial septal defect, persistent ductus arteriosus and interrupted aortic arch. In rarer occasions, AP window has also been documented associating with coronary arterial abnomality, bicuspid aortic valve, pulmonary atresia, subaortic membrane, solitary left superior vena cava (SVC), or aberrant right subclavian artery.3)
There has only been a couple of reported cases of AP window associated with left PA sling. Neither of them was associated with abnormal branching of the bronchi, ventricular septal defect (VSD), and bilateral SVCs.
AP window is treated by surgical closure of the defect. Precise preoperative imaging is essential to recognise the type and the location of the defect. In addition to conventional 2D-echocardiography (2D-Echo), computed tomography (CT) and magnetic resonance imaging (MRI) are of critical importance nowadays to demonstrate associated malformations prior to surgery.
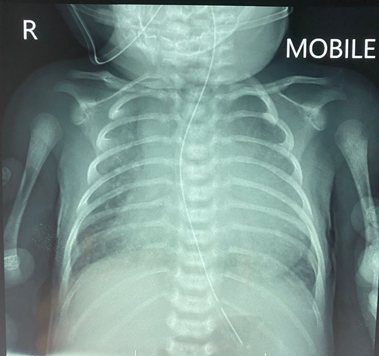
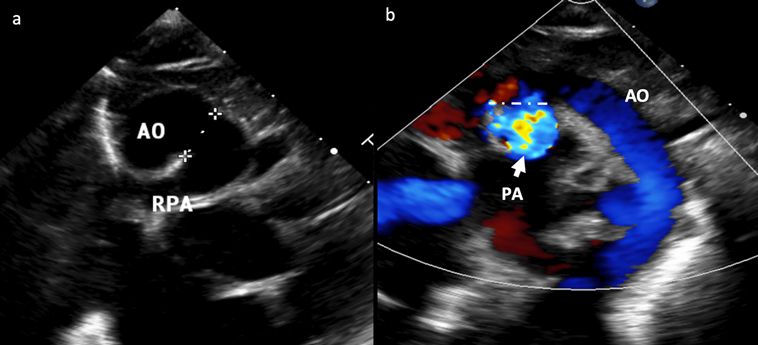
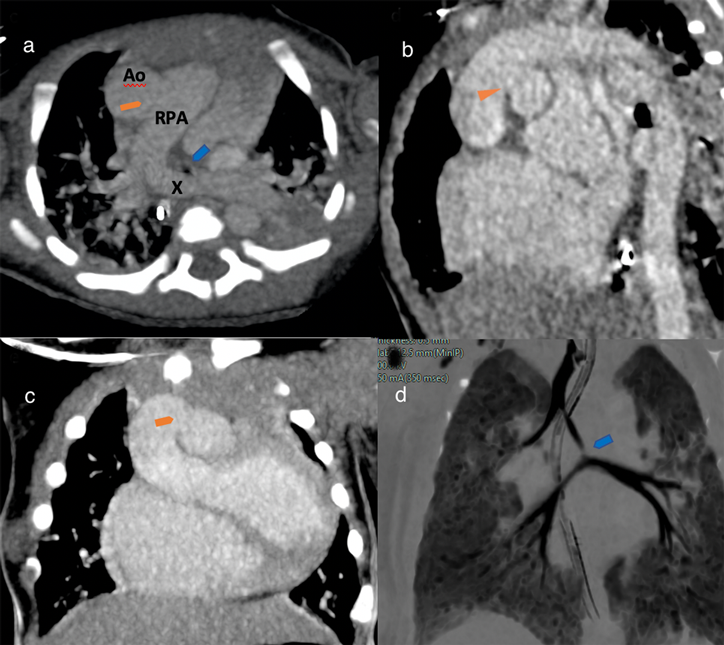
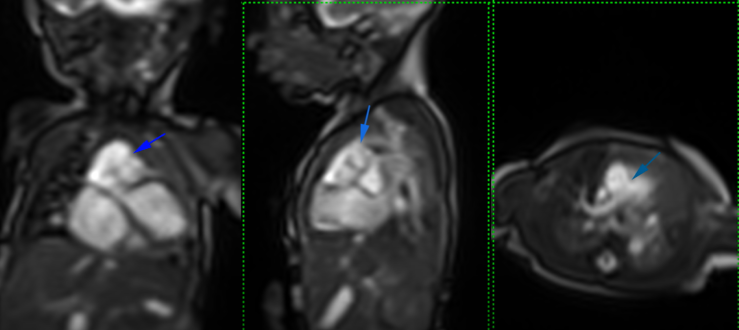
A full-term baby (male, birth weight 3.1 kg) was admitted with signs and symptoms of heart failure, but without cyanosis, at 10 days of life. His pulse oximeter indicated 96% on room air with respiratory rate 56/min, heart rate 147/min, blood pressure 69/35 mmHg. Chest X-ray showed plethoric lung fields and cardiomegaly (Fig. 1). Oxygen was given 1 L/min via a nasal cannula. Frusemide and spironolactone are started. His hemoglobin was 20.0 g/dL, hematocrit 58%, total white blood cells 13,600 µ/L, platelets 181,000 µ/L, CRP 0.1 mg/L, with normal renal function (urea 4.6 mmol/L, Na 133 mmol/L, K 4.5 mmol/L, Cl 95 mmol/L, Ca 2.35 mmol/L). An urgent 2D-Echo showed a large VSD, AP window (Fig. 2) and also PA sling suspected. Thoracic CT angiography confirmed Type 2a PA sling with severe tracheal stenosis. The so-called “tracheal bronchus” gave rise to the right upper lobe; its branching being as if at the usually expected location for the carina. The bifurcation to the right lower lobe and the left lung in this patient was present lower down with abnormal orientation (the bronchi more horizontally oriented than usual). The left PA is located at the T6–7 level just above the carina which resulted in distal airway stenosis (Fig. 3). The SVCs were bilateral structures. Lung volumes appeared fair bilaterally. The coronary arterial origins were normal. Cardiac MRI illustrated the right atrium and the right ventricle dilated, and also reconfirmed PA sling of the left PA as well as AP window between the distal AscAo and the right main PA (Supplementary Movie S1).
This patient became more tachypneic (respiratory rate 68/min) at 15 days old with subcostal recession noted. Venous blood gas showed respiratory acidosis (pH 7.464, pCO2 68 mmHg, pO2 39 mmHg, BE 21.4 mmol/L, HCO3 41.7 mmol/L). He was then intubated and ventilated with low setting ventilation. Arterial blood gas post intubation (pH 7.527, pCO2 31.4 mmHg, pO2 101 mmHg, BE 3.1 mmol/L, HCO3 28 mmol/L). He was transferred to a major cardiac center and eventually underwent successful reimplantation of the left PA, VSD closure and repair of AP window at 38 days of age. Currently, he is well on non-invasive bilevel positive airway pressure.
Supplementary movies are provided online for this article.
謝辞Acknowledgments
We thank the Director General of Malaysian Ministry of Health for the support of this publication.
Statement of Consent
Parents consented to publication of the images and case presentation.
Conflict of Interests
None of the authors have conflict of interest.
引用文献References
1) Mori K, Ando M, Takao A, et al: Distal type of aortopulmonary window: Report of 4 cases. Br Heart J 1978; 40: 681–689
2) Jacobs JP, Quintessenza JA, Gaynor JW, et al: Congenital Heart Surgery Nomenclature and Database Project: Aortopulmonary window. Ann Thorac Surg 2000; 69 Suppl: 44–49
3) Bin-Moallim M, Hamadah HK, Alhabshan F, et al: Aortopulmonary window: Types, associated cardiovascular anomalies, and surgical outcome: Retrospective analysis of a single center experience. J Saudi Heart Assoc 2020; 32: 127–133
 1,Mohd Nizam Mat Bah2,Mohd Hanafi Bin Sapian2,Norliza Othman1Hazrini Abdullah
1,Mohd Nizam Mat Bah2,Mohd Hanafi Bin Sapian2,Norliza Othman1Hazrini Abdullah