The number of newly diagnosed patients with Kawasaki disease (KD) is over 15,000 per year in Japan, and patients with KD are frequently encountered in routine pediatric practice. In the acute phase, approximately 3% of the affected patients develop residual coronary artery enlargement or aneurysm.1) The diagnosis and follow-up of patients with coronary artery enlargement are performed in accordance with guidelines.2) Pediatricians consider KD as the most important cause of coronary artery enlargement or aneurysm in pediatric patients.
However, congenital coronary artery anomalies are the most common causes of coronary artery enlargement and aneurysms. Congenital coronary artery anomalies are classified into four major categories: (1) anomalies in the origin and shape of the coronary artery, (2) stenosis or closure of the coronary artery opening, (3) anomalies in the coronary artery vessel itself, and (4) anomalies in the terminal end of the coronary artery. The definition of congenital coronary artery anomalies differs based on the structure/course of the coronary arteries; however, their incidence is not rare (approximately 1% frequency).3) Further, some of the congenital coronary artery anomalies such as anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) can lead to myocardial infarction, arrhythmia, and heart failure leading to a poor prognosis. Therefore, congenital anomalies of the coronary arteries should be considered when coronary artery enlargement or aneurysm is observed.4, 5)
Here, we report the case of a child with ALCAPA, who was originally diagnosed with right coronary artery enlargement in the acute phase of KD and had been on follow up at a local hospital. We believe that children with coronary artery enlargement or aneurysm should not be diagnosed prematurely as the complication of KD; further, echocardiography and electrocardiography should be performed to differentiate congenital coronary artery anomalies such as ALCAPA.
A 6-year-old girl was referred to our hospital for the evaluation of an enlarged coronary artery. Her history included typical KD diagnosed at the age of 3 years and 1 month. The patient had 6 of the 6 primary symptoms and was successfully treated with intravenous immunoglobulin infusion at day 8 of illness. During the acute phase of KD, dilation of segment 1 of the right coronary artery (2.7 mm in diameter), mild mitral regurgitation, and small patent ductus arteriosus were detected on day 4 of illness. Since then, the patient was on regular follow up at the outpatient clinic.
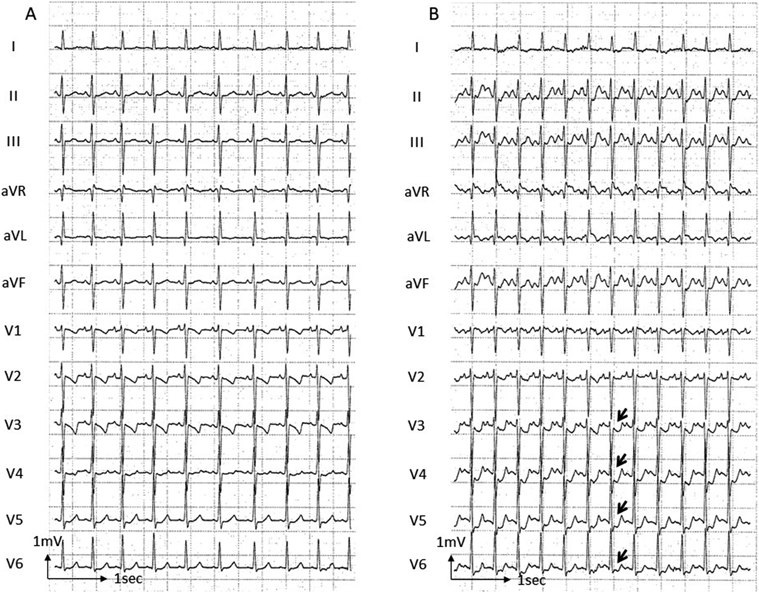
However, at the age of 5, she began to complain of chest pain when running at full speed. The chest pain was located in the mid-chest area and resolved spontaneously in a few minutes on resting. Echocardiography showed an increase in the size of segment 1 of the right coronary artery (3.0 mm at 4 years of age vs. 3.5 mm at 5 years of age). At the age of 6 years and 4 months, she was tentatively diagnosed with coronary artery fistula based on the dilation of the right coronary artery and abnormal flow into the pulmonary artery. The patient underwent a treadmill exercise electrocardiogram (Fig. 1) that revealed 0.1–0.2 millivolt ST-segment depression in leads V3–V6 with no complaints of chest pain. The patient was then referred to us for further cardiac evaluation.
The patient did not have any other significant history and had no family history of the disease.
On examination, the patient’s height and weight were normal{107.7 cm [−1.7 standard deviation (SD)] and 18.2 kg (−0.9 SD), respectively}. Vital signs were within the normal range (heart rate, 83 beats per minute; blood pressure, 94/65 mmHg; and respiratory rate, 20 per minute). There were no abnormal findings on physical examination and on chest auscultation.
Laboratory investigation showed mildly increased NT pro-BNP (174.6 pg/mL); however, CK was normal (85 U/L). The remaining routine laboratory tests were within the normal range.
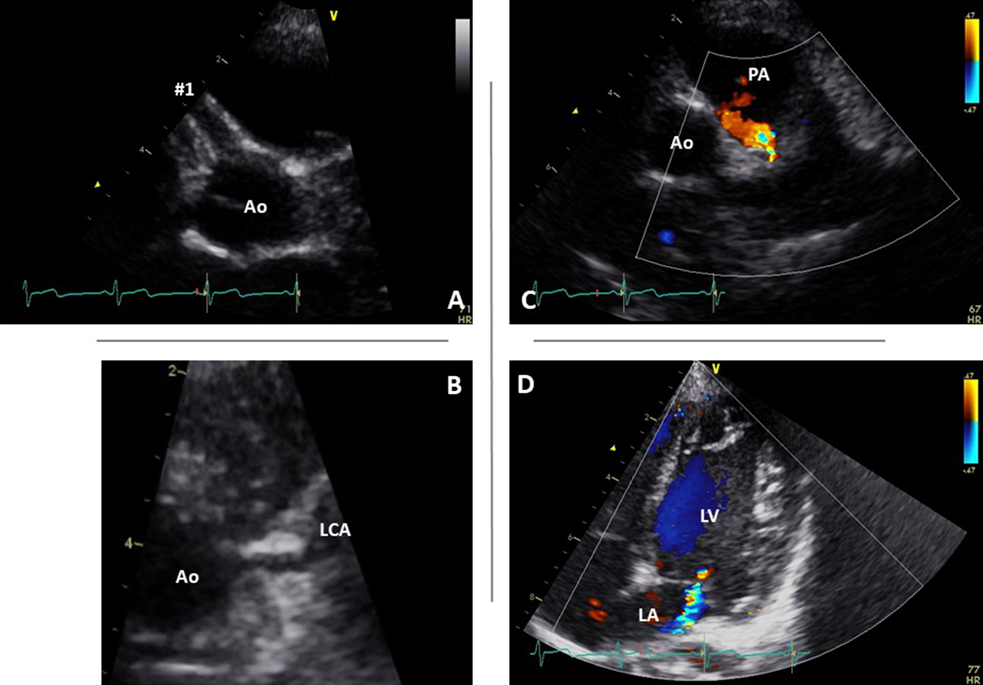
Chest radiograph showed normal cardiothoracic ratio of 49% and there was no lung congestion. A resting 12-lead electrocardiogram showed normal sinus rhythm at 97 beats per minute, mild left axis deviation, normal PQ interval, and negative T wave in aVL. However, there were no abnormal Q waves in any lead and no arrhythmias present. Echocardiography (Fig. 2) showed normal left ventricular end-diastolic dimension [35.1 mm (+0.6 SD)] with normal ejection fraction of 75% without asynergy and mild mitral regurgitation without apparent prolapse. The right coronary artery was further dilated [segment 1, 4.6 mm (+6.7 SD); segment 2, 3.3 mm; and segment 3, 1.6 mm]; however, the left coronary artery was within normal range [segment 5, 2.3 mm (+0.2 SD)]. Although the origin of the left coronary artery appeared normal on B-mode echocardiography (Fig. 2B), the normal forward flow of the coronary artery was not documented.
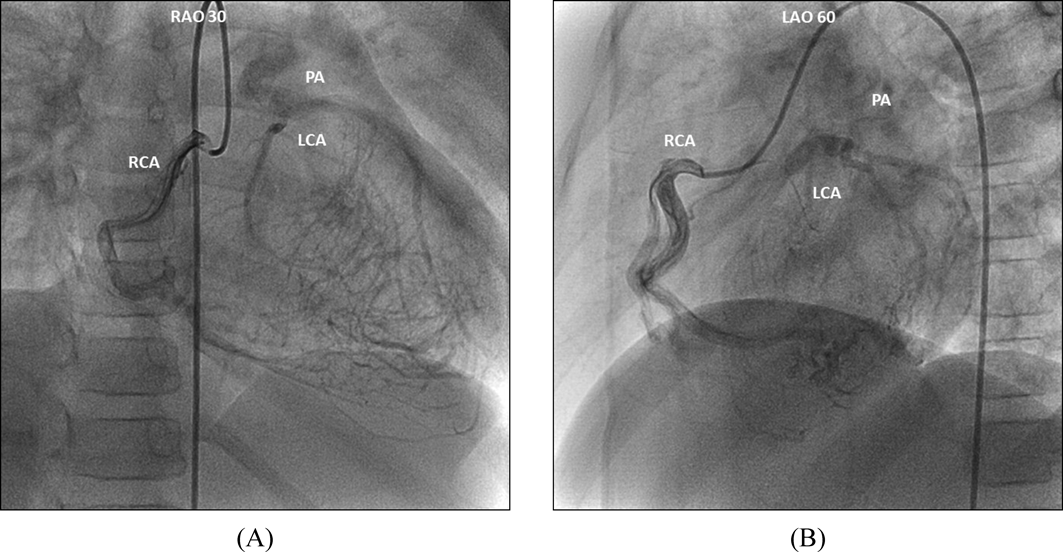
Coronary X-ray computed tomography showed the left coronary artery originated from the pulmonary artery indicating the diagnosis of ALCAPA. Cardiac catheterization and coronary angiography (Fig. 3) of the right coronary artery showed peripheral collateral vessels connecting the left coronary artery; thereby, confirming the presence of retrograde blood flow in the left coronary artery. Mild hypokinesia was observed in the anterolateral wall of the left ventricle. Further, the left ventricular end-diastolic volume was mildly increased to 138% of the normal and the left ventricular ejection fraction was 68%. Adenosine stress myocardial perfusion scintigraphy showed widespread perfusion defect in the anterior to anterolateral walls of the left ventricular myocardium during stress with no reperfusion in some regions, mainly in those supplied by the diagonal branches of left anterior descending artery. Although the patient had limited symptoms, some regions of the myocardium had already lost viability. After 2 months the patient underwent surgical correction to prevent the sudden death. The orifice of the left coronary artery was located very close to the aorta in the middle of the left facing cusp of the pulmonary artery. The left coronary artery was dissected and grafted directly into the aorta. The postoperative course was uneventful, and coronary angiography performed 2 months after the surgery showed smooth blood flow from the aorta to the left coronary artery without stenosis. The patient currently receives outpatient care at our department.
In this report, we present the case of a 6-year-old child with ALCAPA who had been diagnosed and managed at a previous local hospital as a case of right coronary artery enlargement associated with acute stages of KD. When coronary artery enlargement is detected by echocardiography in the early stage of KD, congenital coronary artery anomalies should be included in the differential diagnosis. One of the factors for the misdiagnosis of enlarged coronary arteries due to KD was that the left coronary artery appeared to have a normal origin from the aorta on echocardiography. In fact, it is not uncommon in ALCAPA for the left coronary artery to appear to originate normally from the aorta on echocardiography. Therefore, to differentiate ALCAPA, not only should the continuity between the aorta and the left coronary artery be observed in B-mode, but also the direction of blood flow in the left coronary artery and the presence or absence of blood flow into the pulmonary artery should be confirmed by color Doppler.6, 7) If the origin of the coronary artery is not clear, looking at the left ventricular myocardium with low-speed color Doppler will reveal abnormal signals from many collateral blood vessels draining from the right coronary artery to the left coronary artery, leading to a suspicion of ALCAPA-related disease.8) In this case, the coronary artery appeared to originate from the left coronary cusp, but we were able to confirm the retrograde blood flow into the pulmonary artery. In addition, many abnormal collateral signals from the right coronary artery were observed in the retrospective echocardiographic review.
Moreover, mitral regurgitation is often seen in ALCAPA. In retrospect, enlarged right coronary artery, patent ductus arteriosus-like blood flow, and mitral regurgitation were observed at the time of the first visit to the previous physician, and a detailed echocardiography should have been performed with ALCAPA in mind. Further, the electrocardiogram showed Q waves on aVL that implied myocardial ischemia, which is one of the findings in ALCAPA. Furthermore, the progressive enlargement of the right coronary artery, as observed in this case, is unusual for coronary artery enlargement due to KD: The coronary artery enlargement was observed on the day 4 of illness with no regression during the course of the disease; instead, the enlargement further progressed when the patient was 6 years old. Therefore, our case suggests that apart from KD, congenital coronary artery anomalies should also be considered as causes of coronary artery enlargement.
ALCAPA is an ischemic heart disease involving the left coronary artery. Early diagnosis is important because untreated ALCAPA can lead to myocardial infarction, heart failure, ventricular arrhythmia, and sudden death.9–11) In this case, the diagnosis of ALCAPA was made when the patient was 6 years old. Although some regions of the myocardium had already lost viability, the function of the left ventricle was well-preserved, and there were no arrhythmias involved. Revascularization of the left coronary artery was performed without any complications, and the patient is expected to have a good prognosis.
Here, we report the case of a child with ALCAPA, who was previously misdiagnosed as right coronary artery enlargement due to KD. Treadmill electrocardiography and stress myocardial perfusion scintigraphy showed extensive myocardial ischemia in the areas perfused by the left coronary artery, and corrective surgery was performed. If coronary artery enlargement is observed at an early stage of KD, echocardiographic examination should be performed carefully considering congenital coronary artery malformation as a differential diagnosis.
Conflicts of Interest
None.
Author Contributions
Keitaro Tsuda; drafting of the manuscript and revising it, and final approval of the manuscript submitted.
Shintaro Kishimoto; active involvement in collecting data with subsequent participation in drafting the manuscript.
Yoshiyuki Kagiyama; active involvement in collecting data with subsequent participation in data analysis.
Yusuke Koteda; active involvement in collecting data with subsequent participation in drafting the manuscript.
Kenji Suda; conception and analysis and interpretation of data, revising it critically for important intellectual content, and final approval of the manuscript submitted.
Note
Parts of this paper were presented at the 496th Annual Meeting of the Fukuoka Regional Meeting of the Japanese Pediatric Society (October 21, 2017, Fukuoka).
Originally published in Pediatric Cardiology and Cardiac Surgery, Vol. 35 (2019), pp. 38–42. [in Japanese]
引用文献References
1) Makino N, Nakamura Y, Yashiro M, et al: Descriptive epidemiology of Kawasaki disease in Japan, 2011-2012: From the results of the 22nd national survey. J Epidemiol 2015; 25: 239–245
2) JCS Joint Working Group: Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease (JCS 2013). Digest version. Circ J 2014; 78: 2521–2562
3) Yamanaka O, Hobbs RE: Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990; 21: 28–40
4) Davis JA, Cecchin F, Jones TK, et al: Major coronary artery anomalies in a pediatric population: Incidence and clinical importance. J Am Coll Cardiol 2001; 37: 593–597
5) Kayalar N, Burkhart HM, Dearani JA, et al: Congenital coronary anomalies and surgical treatment. Congenit Heart Dis 2009; 4: 239–251
6) Kudo Y, Suda K, Koteda Y: Pitfalls of echocardiographic evaluation of anomalous origin of the left coronary artery from the pulmonary trunk. Cardiol Young 2008; 18: 537–538
7) Nii M: Congenital coronary anomalies. Pediatr Cardiol Cardiac Surg 2016; 32: 95–113 (in Japanese)
8) Silverman NH: Echocardiographic presentation of anomalous origin of the left coronary artery from the pulmonary artery. Cardiol Young 2015; 25: 1512–1523
9) Yau JM, Singh R, Halpern EJ, et al: Anomalous origin of the left coronary artery from the pulmonary artery in adults: A comprehensive review of 151 adult cases and a new diagnosis in a 53-year-old woman. Clin Cardiol 2011; 34: 204–210
10) Krexi L, Sheppard MN: Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA), a forgotten congenital cause of sudden death in the adult. Cardiovasc Pathol 2013; 22: 294–297
11) Kanoh M, Inai K, Shinohara T, et al: Outcomes from anomalous origin of the left coronary artery from the pulmonary artery repair: Long-term complications in relation to residual myocardial abnormalities. J Cardiol 2017; 70: 498–503
 Keitaro Tsuda, Shintaro Kishimoto, Yoshiyuki Kagiyama, Yusuke Koteda, Kenji Suda
Keitaro Tsuda, Shintaro Kishimoto, Yoshiyuki Kagiyama, Yusuke Koteda, Kenji Suda