Myocardial ischemia is rare in children, but its timely diagnosis is essential, as delayed diagnosis may result in a catastrophic outcome. In adults, ischemic heart disease is the most frequent cause of morbidity and mortality in developed countries. Ischemic heart disease in adults is commonly due to coronary atherosclerosis and may present with recurrent chest pain (angina pectoris) or myocardial infarction as acute events, or with a chronic outcome including ischemic cardiomyopathy and congestive heart failure. Unexpected sudden cardiac death (SCD) is reported in some adult cases of coronary artery disease, especially during exercise.1, 2) In children, coronary atherosclerosis is very rare. Coronary anomalies in children can be classified as either congenital or acquired, and its clinical manifestation is diverse and quite different from that in adults.3, 4) Some coronary anomalies are diagnosed unexpectedly after life-threatening events or sudden death, whereas others present with asymptomatic heart murmur. Although rare, it is imperative for all practitioners to recognize the specific features of coronary anomalies in children; however, a reliable screening strategy for these disorders is currently not available.
In this review article, various coronary anomalies in children are introduced. Then, the underlying cellular pathobiology of myocardial ischemia and its clinical outcome with specific contributing factors are discussed. As an underlying pathological process, acute myocardial ischemia can introduce an ischemic tissue injury resulting in myocardial infarction as well as an electrical instability causing ventricular fibrillation and/or SCD. Lastly, the critical role of mitochondria in modulating pathological pathways in response to myocardial ischemic injury is outlined.
Congenital Coronary Anomalies
Anomalous Left Coronary Artery from Pulmonary Artery
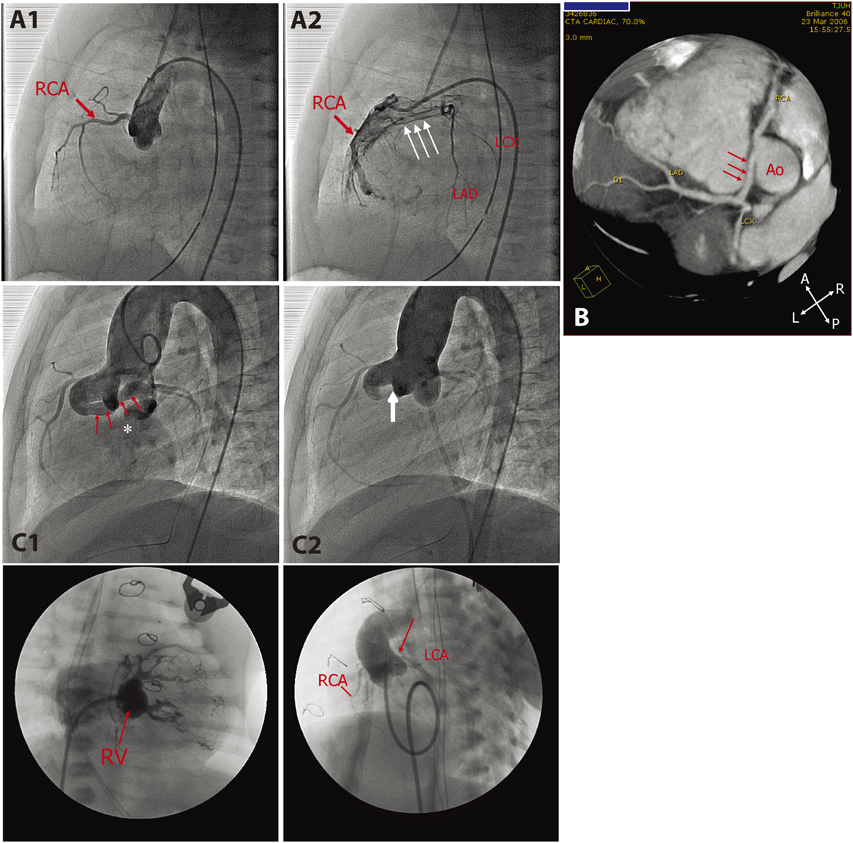
Anomalous left coronary artery from pulmonary artery (ALCAPA) is a rare congenital coronary anomaly typically presenting in infants around 2 to 3 months of age with acute onset of respiratory distress, poor feeding, and paleness secondary to circulatory failure.8–10) These clinical manifestations are attributed to myocardial infarction due to direct myocardial ischemic injury and associated left ventricular (LV) dysfunction and mitral regurgitation (MR). Early diagnosis and prompt surgical intervention (coronary translocation surgery) are essential for the better prognosis (Fig. 1A1, A2). Some infants completely recover LV function after an early diagnosis and a prompt surgical intervention.11–14) It is surprising that infantile myocardium regenerate, even after extensive myocardial damage.15)
Patients with ALCAPA can be totally asymptomatic during childhood. There may be a mild cardiomegaly secondly to the increased left to right shunt with no clinical signs of myocardial ischemia or congestive heart failure. These patients are often encountered in adulthood with difficulty breathing, exercise intolerance, palpitation, chest pain, syncope,16–18) or even SCD.19) Associated late mitral valve insufficiency may complicate a clinical picture of chronic ischemic cardiomyopathy after initial surgical repair in early childhood.12, 20) Diversity of clinical presentation of ALCAPA is thought to depend on the degree of collateral vessel development, the extent of irreversible myocardial ischemic injury and fibrosis, associated hemodynamic abnormalities (pulmonary hypertension,21) large ventricular septal defect,22) patent ductus arteriosus,23) or severe branch pulmonary stenosis24)), and increased myocardial oxygen demand from LV dilatation. ALCAPA includes a clinical spectrum of significant spatiotemporal heterogeneity of myocardial ischemia due to congenital coronary anomaly.
Aberrant Aortic Origin of Coronary Artery
Aberrant aortic origin of coronary artery (AAOCA), another rare congenital coronary anomaly, occurs when the coronary artery arises from the different aortic cusps, consisting of left coronary artery (LCA) from the right aortic cusp and right coronary artery (RCA) from the left aortic cusp. This anomaly is frequently associated with other anatomical abnormalities including interarterial course, intramural course, a slit-like coronary orifice, and an acute angle from the aorta, which are speculated to be the underlying mechanisms of sudden disruption of coronary blood flow at the peak of exercise.25–27) The majority of patients with this condition remain asymptomatic, but the first symptom may be cardiac arrest or SCD, particularly aberrant aortic origin of left coronary artery (AAOLCA)28, 29) (Fig. 1B). AAOLCA is the second most common disease responsible for otherwise healthy young athletes during exercise (first is hypertrophic cardiomyopathy).30) The affected patients seldom experience ischemic chest pain or other warning signs of myocardial ischemia before the fatal event. AAOLCA is generally indicated for surgical intervention (coronary translocation or unroofing of intramural artery) because of a high association with SCD in otherwise healthy individuals.25) The surgical indication for aberrant aortic origin of right coronary artery (AAORCA) remains controversial.31)
The ultimate challenge of AAOLCA is difficulty in identifying this condition before a lethal event, as there are virtually no associated clinical signs or symptoms or laboratory biomarkers other than abnormal coronary imaging studies. The first clinical presentation may be an unexpected SCD. A common encounter of AAOLCA by pediatric cardiologists is either as a coincidental echocardiographic finding for unrelated problems (heart murmur, musculoskeletal chest pain, or nonspecific palpitations, etc.) or as a pathological finding at autopsy for the sudden death victims. Thus far, there is no effective screening method to detect this congenital anomaly.
Coronary Artery Fistula
Coronary artery fistula (CAF) or coronary cameral fistula implies fistulous communication between the existing coronary artery to any of the cardiac chambers (right atrium, left atrium, right ventricle, and left ventricle) or vessels (pulmonary artery)32, 33) (Fig. 1C1, C2). It can be small or enlarged with aneurismal morphology. Usually, CAF is diagnosed in asymptomatic patients with continuous murmur during childhood or clinical signs of left ventricular volume overload in adult patients. Adult patients may present with exercise intolerance or atrial arrhythmia due to volume overload and/or myocardial ischemia secondary to myocardial steal phenomenon.33) Echocardiography with a color Doppler study is usually sufficient to make a diagnosis. In children with asymptomatic CAF, fistula may be electively occluded with closure-device or coils under cardiac catheterization or surgically ligated. Symptomatic adult patients require necessary intervention. An understanding of correct coronary anatomy is crucial for intervention, as postoperative thromboembolic complications are reported.34–36)
Pulmonary Atresia with Intact Ventricular Septum
Variable coronary abnormalities are known to complicate in pulmonary atresia with intact ventricular septum (PA/IVS). Persistent exposure to significantly elevated right ventricular pressure predisposes the development of sinusoidal communication between the right ventricular cavity and existing coronary arteries (Fig. 1D1, D2).37) When this sinusoidal communication becomes predominant, the intrinsic coronary arteries may develop regression, causing proximal coronary stenosis or coronary atresia.38, 39) This condition is called “right ventricle-dependent coronary circulation (RVDCC),” and is responsible for an increased risk of myocardial ischemia or steal phenomenon with RV-decompression surgery or even shunt placement.40–42) This underlying coronary anomaly is responsible for high perioperative morbidity and mortality. It is essential to assess the possibility of RVDCC prior to surgical intervention to minimize the risk of myocardial infarction during and after surgery.43)
Acquired Coronary Anomalies
Acquired conditions that induce coronary abnormalities during childhood include Kawasaki disease and other vasculitis (Takayasu disease44)), coronary artery obstruction after arterial switch operation for transposition of the great arteries, post-transplant allograft vasculopathy, and genetic disorders (William syndrome45)).46) Atherosclerotic coronary disease is rare in children, although it may be seen in adolescents with familial hypercholesterolemia (homozygous type).47)
Kawasaki Disease and Giant Coronary Aneurysm
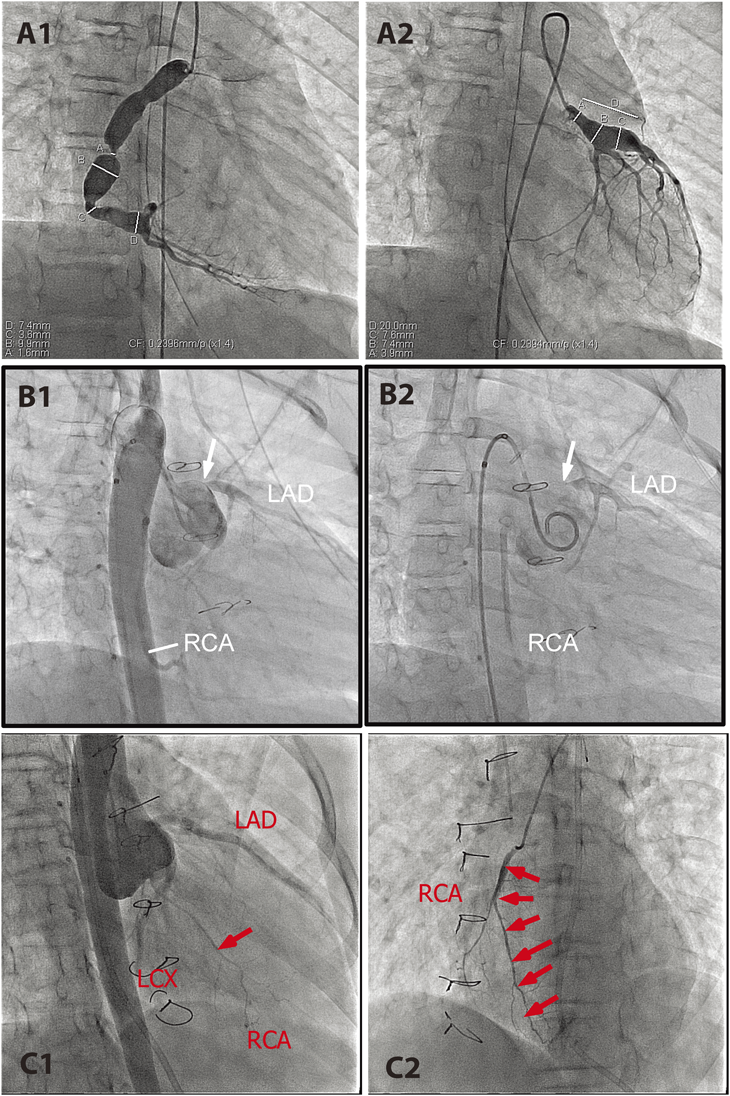
Kawasaki disease is known to cause coronary artery deformation, ectasia, and/or aneurismal formation during and after the acute phase of the disease.48, 49) Coronary aneurysm and secondary coronary stenosis as the results of uneven regression of ectasia are thought to predispose to vascular occlusion (Fig. 2A1, A2). Aneurysms are mainly seen at the proximal coronary arteries or at the bifurcations. Echocardiogram is useful in detecting these coronary lesions that evolve dynamically over time.50) Aneurysm may increase in size over the first 2 months, depending upon the degree of vasculitis, followed by spontaneous regression by 2 years after the onset; however, vascular stenosis progresses over many years.50, 51) Due to the early introduction of high-dose intravenous immunoglobulin (IVIG), the incidence of coronary aneurysm and its complications are dramatically decreased.52, 53) Vascular occlusion by thrombus formation and/or intimal thickening results in myocardial ischemia, infarction, or sudden cardiac death.54) Of 60 patients who developed myocardial infarction following Kawasaki disease, 50% developed within 6 months after the onset. Fifteen patients (25%) died, 3 died during the acute phase, and 12 patients died during the chronic phase. Half of the late deaths (6 patients) were of sudden unexpected death.54) The late sudden cardiac death frequently occurs in asymptomatic patients.55)
d-Transposition of the Great Arteries after Arterial Switch Operation
Arterial switch operation (ASO) is primarily indicated in the newborn period for surgical repair of d-loop transposition of the great arteries (d-TGA) and Taussig-Bing anomaly. Because the procedure involves translocation of the coronary arteries, coronary complications may occur during the acute56, 57) and chronic phases.58–60) While short-term coronary complications are related to intrinsic coronary artery anatomy and surgical procedure per se, long-term complications frequently occur unexpectedly without any associated clinical signs or symptoms58, 61, 62) (Fig. 2B1, B2). Routine ECG, echocardiogram, exercise stress test (EST), and myocardial perfusion imaging (MPI) are neither sensitive nor specific to identify most of preclinical coronary disease.58, 63) Affected patients are usually asymptomatic or unexpectedly present with lethal (sudden death) or near-lethal (ventricular fibrillation) events. Pathological specimens reveal an intimal thickening of obliterated coronary arteries,60, 64) but the underlying mechanism of this process remains largely unknown. The necessity of routine coronary imaging study in post-ASO patients is advocated by certain groups, including the current author, to risk-stratify a preclinical coronary disease after ASO.60, 65, 66)
Cardiac Allograft Vasculopathy
Cardiac allograft vasculopathy (CAV), a diffuse coronary narrowing known to occur in the recipients of heart transplant, is a major risk factor in limiting long-term survival after heart transplantation.67–69) Unlike atherosclerotic coronary disease, CAV causes diffuse narrowing of coronary arteries (Fig. 2C). Histopathologically, CAV is characterized by the proliferation of vascular smooth muscle cells in the allograft and concentric intimal thickening.70) The pathogenesis of diffuse intimal thickening associated is thought to be due to multiple factors including chronic rejection, endothelial dysfunction, infection, and traditional cardiac risk factors (hypertension, hypercholesterolemia, and diabetes mellitus),67, 71) but the precise mechanism is not fully understood. The incidence of CAV in children is less than that in adults, but is known to occur in 5% to 7% within 2 years after transplant and 15% to 18% within 5 years after transplant.72) The prognosis of CAV is poor, as approximately 50% of cases will result in either graft loss or death within 2 years after the diagnosis.72, 73) Clinical presentation is variable and frequently nonspecific, as the affected patients may not complain of typical anginal pain because renervation over the implanted heart is often incomplete.74) The presence of abdominal, chest, and/or arm pain after heart transplant, however, is strongly associated with CAV and sudden death or aborted sudden death.75) The effective treatment or prevention for CAV is currently not known, but new data are emerging that can potentially help control or attenuate the development of pathological vascular remodeling.76)
Clinical Outcome and Underlying Mechanism of Myocardial Ischemia
Clinical manifestations of coronary disease in children are diverse and much different from those in adults. Although rare in incidence, failure to recognize the condition may result in an unexpected catastrophic outcome. Most children with myocardial ischemia do not necessarily complain of ischemic chest pain as a preceding warning symptom. They tend to be asymptomatic until they present abruptly with ventricular fibrillation or unexpected sudden death as a first presentation. SCD in middle-aged athletes presents in a similar way, as they are commonly considered least at risk to develop coronary insufficiency.1) There are two major challenges in managing silent coronary anomalies and preclinical myocardial ischemia in children: 1) difficulty in identifying the population at risk for SCD, and 2) lack of general guidelines in making risk stratification for SCD in patients with silent coronary anomalies.
Clinical Presentation of Myocardial Ischemia in Children
Heterogeneity of the ischemic myocardium and variable different physical conditions may create a diverse clinical spectrum encompassing angina chest pain, ventricular arrhythmia, myocardial infarction, cardiogenic shock, and SCD. SCD due to myocardial ischemia is seen with or without associated myocardial infarction, but usually occurs before the actual myocardial damage becomes evident.77) In other words, upon acute disruption of myocardial perfusion, some patients tolerate initial risk of developing ventricular fibrillation to survive until myocardial infarction develops.77)
Coronary anomalies in children may be classified into two groups based on the outcome of myocardial ischemia. The first, ALCAPA (early infancy), RVDCC in PA/IVS (early infancy), and giant aneurysm in Kawasaki disease (acute and chronic phase), may primarily present with myocardial infarction. The second group, AAOLCA, d-TGA after ASO (long term complication), and CAV, frequently present with unexpected cardiac arrest or SCD without visible myocardial infarction.78) Two cases of unexpected SCD were reported in Kawasaki disease with CA obstruction in a chronic phase.55) Upon myocardial ischemia due to sudden disruption of coronary blood flow, under what mechanisms can these two distinct pathways take place? It is imperative to understand the predisposing factors that favor ischemic myocardium developing into VF before having tissue injury.
Pathobiology of Myocardial Ischemia
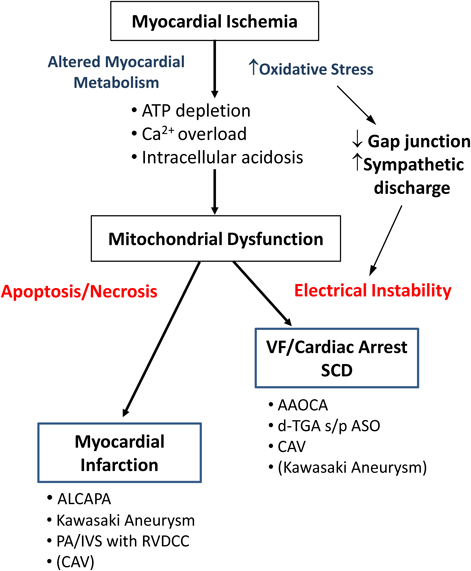
The heart is a highly energy-demanding organ that supports continuous dynamic pumping activity, in which oxygen delivery via coronary circulation plays a vital role. Sudden disruption of coronary blood flow causes myocardial ischemia, resulting in a mismatch between supply and demand of oxygen. Persistent disruption of myocardial perfusion not only induces energy depletion in each myocyte but also compromises washout of metabolic substrates generated by an anaerobic metabolism. As a result, ischemic myocytes develop intracellular acidosis, calcium overload, loss of gap junction function, irreversible cellular injury, increased oxidative stress, accumulation of reactive oxygen species (ROS), and mitochondrial dysfunction.79) These initial myocyte changes are responsible for two major pathological pathways: an electrical instability causing ventricular fibrillation (VF) and actual myocardial damage by cell death program (apoptosis and necrosis) (Fig. 3). Reperfusion following ischemia is primarily beneficial to reverse myocytes at risk, but it can be detrimental by introducing enhanced inflammatory responses inducing additional myocardial damage (ischemic-reperfusion injury).80) VF is an ominous condition, frequently responsible for SCD following myocardial ischemia.
Several other factors may affect the fate of myocardium upon sudden disruption of coronary perfusion, including preconditioning, autonomic nervous system involvement, degree of collateral vessel development, and associated physical condition (e.g., exercise, emotional stress, cold weather). Preconditioning, a repetitive exposure of mild ischemic stress and reperfusion to enhance myocardial adaptation, is known to protect against greater subsequent ischemic insults with less threat of infarction81) and VF.82) Increased sympathetic discharge in association with pain, fear, and emotional outrage by sudden ischemia increases a risk of ventricular fibrillation or progression of direct myocardial injury.83) In an experimental myocardial infarction by left coronary artery ligation in the rat model, the incidence of sudden death was significantly higher under conscious sedation than under general anesthesia, suggesting detrimental effects induced by pain and associated sympathetic discharge.84) In ischemia-induced VF, sympathetic activation is considered proarrhythmic, whereas parasympathetic activation is antiarrhythmic.85) Targeted ablation of cardiac sympathetic neurons significantly reduced the susceptibility to ischemia-induced ventricular tachycardia in conscious rats.86) Active involvement of the autonomic nervous system in various cardiovascular diseases, including myocardial ischemia-induced SCD, was recently reviewed by Fukuda et al.87) Another important factor is collateral vessel formation or arteriogenesis, which is based on growth and remodeling of preexisting collateral anastomoses.88) The degree of collateral vessel development determines the myocardial integrity by increasing the threshold of electrical instability and cardioprotection against direct ischemic injury.89, 90) Preconditioning certainly enhances collateral vessel development, but the precise mechanism of arteriogenesis by ischemia is not fully understood.91) The overall net myocardial perfusion through obstructed native coronary arteries and the presence of collateral vessels may determine the final clinical outcome upon major ischemic events. Chronic myocardial ischemia commonly seen in ALCAPA, Kawasaki disease, or PA/IVS with RVDCC tends to stimulate collateral vessel formation, whereas AAOCA does not. The presence of collateral vessels increases cardioprotection against SCD,92) which has also been shown in CAV.93) Lastly, physical activities trigger SCD in coronary artery disease in older adults; this is more common in males and during heavier exercise.94) On the contrary, Reddy et al. reported that 80% of SCD occurred with light physical activities or during sleep rather than moderate to heavy exercise in older patients.95) The effects of exercise on SCD candidates are complex, as light to moderate regular exercise is proven to enhance cardioprotection against ischemic heart disease.96)
Mitochondria, a Critical Site of Regulating Myocyte Homeostasis
The Mitochondrion is an energy-converting machinery of cells that regulates metabolism via the Krebs cycle and electron-transport chains. Continuous vigorous myocyte contractile activity is highly dependent upon ATP generated by oxidative phosphorylation in the mitochondria with constant oxygen supply. In addtion to oxidative phosphorylation and ATP synthesis, mitochondria play a critical role in the regulation of Ca2+ and reactive oxygen species (ROS)-mediated processes in the myocytes.97, 98) Myocardial ischemia imposes multiple biological insults on mitochondria. As a result, hearts develop electrical instability responsible for VF and/or direct tissue injury through apoptosis and necrosis (oncosis) to induce myocardial infarction.99) Myocardial mitochondria play a vital role in determining which critical pathway to take in response to overwhelming ischemia. How can the energetic status of the mitochondrial network induce the myocardial electrical instability to cause VF and/or cell death signaling pathways to result in myocardial infarction?
Ischemia-induced oxidative stress alters the cardiac mitochondrial network and thus induces spatiotemporal action potential heterogeneity. This action potential heterogeneity causes lethal ventricular arrhythmia via multiple different levels including sarcolemmal ATP-sensitive potassium channel (sarcKATP), mitochondrial inner membrane anion channel (iMAC), mitochondrial permeability transition pore (mPTP), mitochondrial ATP-sensitive potassium channel (MitoKATP), and mitochondrial calcium uniporter.100) Regional mitochondrial depolarization triggered by oxidative stress activates sarcKATP to initiate electrical propagation by forming metabolic sink.101) Instability of iMAC is linked with heterogeneous electrophysiological substrate of the post-ischemic heart.102) Persistent mPTP opening is accompanied by mitochondrial depolarization and massive swelling due to an influx of ions and water into the matrix, which results in cell death via apoptotic and necrotic pathways.97) In addition, ischemia-induced intracellular acidosis and Ca2+ overload alter the conductance at gap junctions, which also contributes to electrical heterogeneity.82, 103) The expression of gap junction protein, connexin 43, is shown to be downregulated with myocardial ischemia.104, 105) Myocardial ischemia induces a complex cascade of events generating a diverse clinical presentation of cardiac rhythm abnormality and myocardial tissue injury through mitochondria.98)