Since Kawasaki disease (KD) was reported in 1967, some patients have been known to develop coronary arterial lesions (CALs).1, 2) Various treatments for KD show some promise in decreasing likelihood of subsequent CALs.3–7) For now, however, the number of patients with CALs emerging after KD has been increasing, which possesses a serious clinical problem. Calcified CALs following KD are of great concern, since a calcified stenotic lesion is known to increase risk of coronary artery events.8) We hypothesized that the composition of coronary arterial calcifications following KD might differ from that of atherosclerotic calcifications because KD-associated lesions occur at an earlier age, and that we might better prevent cardiac events following KD if we understood the differences.9)
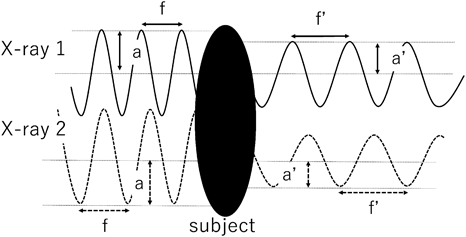
Recently, dual-energy computed tomography (CT) has been used to determine the composition of materials. Dual-energy CT is an imaging method using X-rays with 2 different energy levels to obtain the difference in attenuation coefficients for the material examined. This approach allows us to determine effective atomic numbers (EANs) of materials. When X-rays penetrate a subject, X-ray amplitude and frequency change (Fig. 1). The ratio of changes in amplitude and frequency is characteristic with an element. EAN is an atomic number of this element which is defined with the ratio of changes.10) Human studies concerning EANs of teeth, urinary stones, and atherosclerotic coronary arterial calcifications have been reported.11–13) The EAN of atherosclerotic coronary arterial calcifications was 13.8±0.8, close to that of calcium oxalate monohydrate (13.8).11) However, we know of no similar reports dealing with the composition of coronary arterial calcifications that can follow KD.
In this study we used dual-energy CT to determine the compositions of such coronary arterial calcifications.
A retrospective search of clinical records at our hospital for patients who had undergone dual-energy CT to evaluate CALs following KD between February 2014 and December 2015 identified 25 individuals. Dual-energy CT is performed with a prospective ECG-gated step and shoot technique, so patients who cannot hold their breath or still have a heart rate exceeding 70 beats per minute after beta-blocker administration undergo ECG-gated helical CT rather than dual-energy CT. We excluded 14 patients, 9 patients did not have a calcification exceeding 1 mm and 5 patients’ raw data had been erased.
Among the 11 patients studied, 9 were male and 2 were female. The age of KD onset ranged from 3 months to 6 years (median, 3 years). The age when dual-energy CT was performed ranged from 15 to 45 years (median, 36 years). A total of 23 CALs were studied, including 14 in the right coronary artery and 9 in the left coronary artery (4 in the left main coronary trunk and 5 in the left anterior descending artery). Six patients experienced coronary arterial events (the past-history of acute myocardial infarction or coronary artery bypass grafting). Three of them underwent coronary artery bypass grafting, while 2 experienced acute myocardial infarction; 1 of these patients had infraction and bypass grafting. In the acute phase of KD, 4 patients were given intravenous immunoglobulin, while 1 patient received a corticosteroid. For 6 patients, details about treatment in the acute phase are not known because treatment was carried out at other hospitals. No patient had a history of hypertension, diabetes, administration of warfarin (which can promote coronary arterial calcification), or smoking.14) Only one patient had hyperlipidemia. Patient profiles are described in Table 1.
Table 1 Patient profiles| Patient | Gender | Age at KD onset | Age at imaging | Number of CALs (number in RCA) | CAE† | Treatments during acute period | Other risk factors |
|---|
| 1 | M | 11 months | 15 years | 1 (0) | CABG | Aspirin+IVIG + UTI | None |
| 2 | M | 4 years | 17 years | 1 (1) | None | Aspirin+IVIG | None |
| 3 | M | 6 years | 18 years | 1 (1) | CABG | Aspirin+IVIG + UTI | None |
| 4 | M | 4 years | 25 years | 2 (1) | None | Aspirin+IVIG | None |
| 5 | M | 3 months | 34 years | 3 (2) | CABG | Unknown | None |
| 6 | M | 3 years | 36 years | 3 (2) | AMI, CABG | Unknown | None |
| 7 | M | 5 years | 36 years | 4 (3) | None | Unknown | None |
| 8 | M | 5 years | 37 years | 2 (1) | AMI | Unknown | None |
| 9 | F | 1 year | 38 years | 1 (0) | None | Unknown | None |
| 10 | F | 2 years | 39 years | 2 (1) | None | Unknown | Hyperlipidemia |
| 11 | M | 1 year | 45 years | 3 (2) | AMI | Corticosteroid | None |
| Median | | 3 years | 36 years | 2 | | | |
M, male; F, female; KD, Kawasaki disease; CAL, coronary arterial lesion; RCA, right coronary artery; CAE, coronary arterial event; AMI, acute myocardiac infarction; CABG, coronary artery bypass grafting; IVIG, intravenous immunoglobulin; UTI, ulinastatin.
†The past-history of acute myocardial infarction or coronary artery bypass grafting. |
The imaging device used was Discovery CT750HD FREEdom Edition (GE Healthcare Japan, Tokyo, Japan).
Before scanning, the patient was initiated in an intravenous drip forearm. A scout scan and a simple radiographic image, (a single-energy CT) were obtained to determine the imaging range. An intravenous contrast agent was injected (0.8 to 1.0 mL/kg) over 13 seconds, regardless of patient weight; then cardiac dual-energy CT was performed. Before the dual-energy scan, nitroglycerin (isosorbide spray, 1.25 mg to the oral cavity) was administered as a pre-treatment. When the heart rate was elevated, a beta-blocker (landiolol, 0.125 mg/kg) was given intravenously before the scanning.
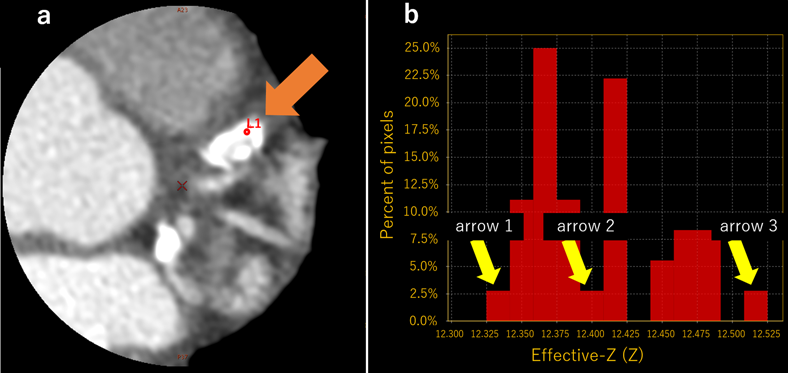
AW VolumeShare5 Plus XT for FREEdom (GE Healthcare Japan, Tokyo, Japan) was used to manipulate images. We adjusted the field of view to 6.0 cm to include mainly calcified lesions. Using the work station, randomly we selected 3 regions of interest (ROI); each 0.7 mm in diameter within the calcification (Fig. 2). An EAN value was obtained for each pixel. With constriction of the field of view, image resolution increased while numbers of pixels and numbers of EAN values for the ROI also increased. We obtained 36 EAN values per 1 ROI, then calculating average values constructing histograms of the distributions of the median, minimal, and maximal EANs of each ROI. In addition, we compared the median EANs of groups defined by features; fenders, coronary arterial events, age at KD onset, years from onset of KD to imaging, and number of CALs.
Statistical analysis was performed using IBM SPSS Statistics 22. The t-test was used to examine the comparison between 2 groups. A p value less than 0.05 was considered to indicate statistical significance. Continuous variables were expressed as mean±SD or median (interquartile range), as appropriate.
This study was approved by the Institutional Review Board of Kindai University, Faculty of Medicine (28-139).
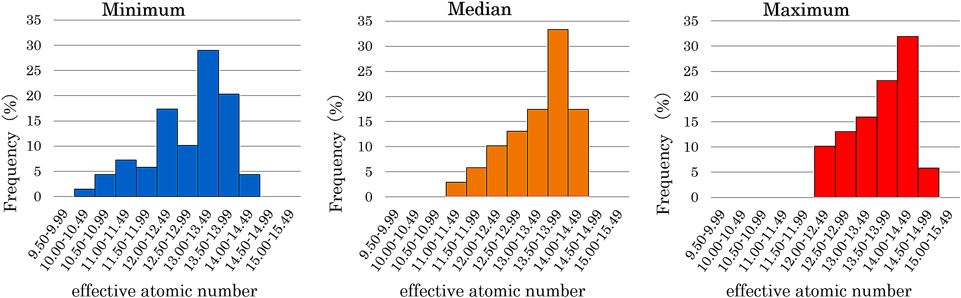
We obtained 2484 EAN values from 69 ROIs. The mean of the median EANs of ROIs was 13.27±0.83, while that of the minimum EANs was 12.80±0.93 and that of the maximum EANs was 13.59±0.72. The median was similar to the EAN of atherosclerotic coronary arterial calcifications (13.8±0.8). The histograms are presented in Fig. 3. According to the results, it suggested that these values did not have large differences.
Analysis of each ROI (Table 2) showed significant differences between groups defined by age at KD onset (<1 year, 13.77±0.55 vs ≧1 year, 13.16±0.80, p<0.01). This suggested that when KD occurred at an age of less than 1 year, EANs more closely resembled those seen in atherosclerosis. EANs showed no differences related to gender, coronary arterial events, years since onset of KD, or number of CALs.
Table 2 Comparison of median EANs according to patient characteristics | | n | EAN | p |
|---|
| Gender | M | 60 | 13.27±0.83 | 0.504 |
| F | 9 | 13.23±0.52 |
| Age at KD onset | <1 | 12 | 13.77±0.55 | <0.01 |
| ≧1 | 57 | 13.16±0.80 |
| Interval (years) between KD onset and imaging | <32 | 27 | 13.47±0.62 | 0.142 |
| ≧32 | 42 | 13.13±0.87 |
| Number of CAL | <2 | 12 | 13.45±0.55 | 0.618 |
| ≧2 | 57 | 13.23±0.84 |
| M, male; F, female; KD, Kawasaki disease; CAL, coronary arterial lesion; EAN, effective atomic number. |
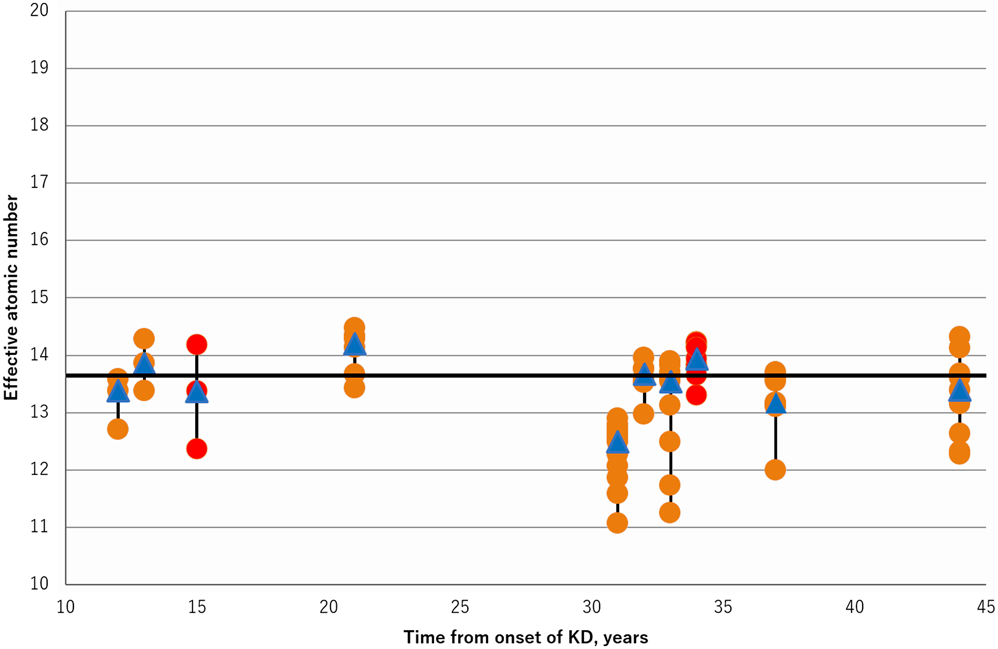
Fig. 4 shows the relationship between years since onset of KD and median EANs. Median EANs were similar to EANs of atherosclerotic coronary arterial calcifications (13.8), irrespective of the time since KD onset.
Calcification in CALs following KD is clinically significant, considering that calcification is a risk factor for coronary arterial events.15) The composition of this calcification has not been reported previously, even in pathological studies. We hypothesized that the calcifications of CALs following KD might differ from those in atherosclerosis, but EANs of KD-related coronary arterial calcifications showed compositions resembling those in atherosclerosis.
In atherosclerotic lesion, chronic mild endothelial injury results from hypercholesterolemia, inflammation, and sometimes exposure to tobacco smoke constituents. As a results, endothelial cell function decreases.16, 17) Ensuring events include inflammation with monocyte recruitment, smooth muscle cell proliferation, accumulation of lipid-laden macrophages, and formation of cholesterol crystals; constitutes an atheroma.17) Gradually, calcification then ensures. Some details of this process remain incompletely understood.18)
In the acute phase of KD, on the other hand, cells such as monocytes, macrophages, and neutrophils infiltrate into coronary arteries from the lumen and adventitia, until inflammation extends through all layers of the coronary artery.19, 20) As a result, vascular smooth muscle, the internal elastic lamina, and extracellular matrix, —all important in maintaining arterial structure—, are injured and CALs develop.21) Coronary arterial calcifications seen 40 or more days after onset of KD have been thought to follow cicatrization of disordered and necrotic tissue in the walls of coronary arteries—i.e., dystrophic calcification— or alternatively, organization of a thrombus. As with atherosclerosis, however, mechanisms of coronary arterial calcification after KD are not fully evident.9)
Pathological studies late in the course of KD have described hyalinized fibrous tissue, lamellar calcification, intimal thickening and lesions like progression of CALs resembling that in atherosclerosis.22, 23) Furthers even late in the evolution of CALs following KD, sustained chronic inflammation was considered to increase risk of atherosclerosis.24, 25) Therefore, atherosclerosis is expected to occur readily in CALs following KD, even though pathogenetic triggers and speeds of progression of calcification seem likely to differ. Mechanisms of progression are likely to overlap, and we found compositions of calcifications to be essentially the same.
Even for calcifications occurring in the patients whose age at KD onset was less than 1 year, EANs resembled those in atherosclerosis. When the acute stage of KD runs its course in less than 1year, inflammation tends to be more severe, requires more aggressive treatments.4, 26) Furthers, even in CALs examined long after KD, slight inflammation persists.24) We suspect that inflammatory cytokines persist longer and at higher levels when inflammation was more intense in the acute phase. Chronic sustained inflammation has been identified as a risk factor for atherosclerosis and arterial calcification, particularly when serum interleukin-6, 8, and 13 were high.24, 27) When the age at KD onset was less than 1 year, patients who develop CALs after the acute stage might be suspected to develop atherosclerosis and calcification more rapidly. We suggest that in the year following onset of KD, stronger anti-inflammatory agents may be needed, and if CALs then still occur, a period of continuing-treatment will be needed, such as aspirin at 30 mg/kg. We believe that when possible, warfarin should be avoided for late-treatment because of a report associating such treatment with increased calcification in a population with atherosclerosis.28)
As depicted in Fig. 3, the EANs in calcifications following KD resembled those in coronary arterial calcifications caused by atherosclerosis (13.8), regardless of duration. We believe that the KD-related lesions progressed like purely atherosclerotic ones and that calcification often progressed over as many as 10 years following onset of KD, while progression rare remained steady regardless of duration. We therefore maintain that patients found to have CALs after the acute phase of KD require treatments aiming to prevent progression of atherosclerosis.
Unfortunately, more risk factors for occurrence of progression of coronary arterial calcification following KD remain to be determined. We intend to study these patients and additional ones over a longer time in the future.
Study Limitations
ROIs were placed by the first author alone. The number of patients was relatively small and ages of patients varied. We were concerned that EANs might have been skewed had numbers of investigators placing ROIs been large. In addition, treatments in the acute phase varied between patients as did the interval from KD onset to performance of imaging. Moreover, we did not have the data of inflammation markers in acute phase. These factors might have influenced the apparent speed of progression. However, EANs in calcifications varied little. Sequential examinations may be desirable.
We examined the composition of coronary arterial calcifications following KD based upon EAN. Composition of these calcifications resembled those in atherosclerosis irrespective of other risk factors, so vigilance against early coronary arterial events is required following KD.
Conflict of Interests
Nobuyoshi Kusano, Noboru Inamura, Satoshi Marutani, Tohru Shinohara, and Tsukasa Takemura received a research grant from GE healthcare Japan.
略語Abbreviations
| KD | Kawasaki disease |
|---|
| CT | computed tomography |
|---|
| EAN | effective atomic number |
|---|
| ROI | region of interest |
|---|
| CAL | coronary arterial lesion |
|---|
引用文献References
1) Kawasaki T: Febrile oculo-oro-cutaneo-acrodesquamatous syndrome with or without acute non-suppurative cervical lymphadenitis in infancy and childfood: Clinical observations of 50 cases. Arerugi 1967; 16: 178–222 (in Japanese)
2) Nakamura Y, Aso E, Yashiro M, et al: Mortality among persons with a history of Kawasaki disease in Japan—Mortality among males with cardiac sequelae is significantly higher than that of the general population—. Circ J 2008; 72: 134–138
3) Miura M, Kohno K, Ohki H, et al: Effects of methylprednisolone pulse on cytokine levels in Kawasaki disease patients unresponsive to intravenous immunoglobulin. Eur J Pediatr 2008; 167: 1119–1123
4) Kobayashi T, Saji T, Otani T, et al: Efficacy of immunoglobulin plus prednisolone for prevention of coronary artery abnormalities in severe Kawasaki disease (RAISE study): A randomized, open-label, blinded-endpoints trial. Lancet 2012; 379: 1613–1620
5) Mori M, Imagawa T, Hara R, et al: Efficacy and limitation of infliximab treatment for children with Kawasaki disease intractable to intravenous immunoglobulin therapy: Report of an open-label case series. J Rheumatol 2012; 39: 864–867
6) Kanai T, Ishiwata T, Kobayashi T, et al: Ulinastatin, a urinary trypsin inhibitor, for the initial treatment of patients with Kawasaki disease: A retrospective study. Circulation 2011; 124: 2822–2828
7) Suzuki H, Terai M, Hamada H, et al: Cyclosporin A treatment for Kawasaki disease refractory to initial and additional intravenous immunoglobulin. Pediatr Infect Dis J 2011; 30: 871–876
8) Tsujii N, Tsuda E, Kanzaki S, et al: Late wall thickening and calcification in patients after Kawasaki disease. J Pediatr 2017; 181: 167–171.e2
9) Kosuda T, Sone K, Kobayashi T, et al: Clinical study of mucocutaneous lymph node syndrome associated with the calcification of coronary arteries. Acta Cardiol Pediatr Jpn 1991; 7: 269–275
10) Matsumoto M, Takayama N: Material identification from C-ray images made with energy-differentiation type radiation line sensor. Bull Soc Photogr Imag Japan 2009; 72: 399–405 (in Japanese)
11) Matsui K, Machida H, Mitsuhashi T, et al: Analysis of coronary arterial calcification components with coronary CT angiography using single-source dual-energy CT with fast tube voltage switching. Int J Cardiovasc Imaging 2015; 31: 639–647
12) Suzuki Y, Shimano T: The effective atomic number of the teeth. Dental Radiol 1976; 16: 1–10 (in Japanese)
13) Ogawa N, Sato S, Ida K, et al: Evaluation of urinary stone composition and differentiation between urinary stones and phleboliths using single-source dual-energy computed tomography. Acta Med Okayama 2017; 71: 91–96
14) Blaha MJ, Budoff MJ, DeFilippis AP, et al: Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: Implications for the JUPITER population from MESA, a population-based cohort study. Lancet 2011; 378: 684–692
15) Fuster V, Badimon L, Badimon JJ, et al: The pathogenesis of coronary artery disease and the acute coronary syndromes. N Engl J Med 1992; 326: 242–250
16) Hori T, Matsubara T, Ishibashi T, et al: Relationsip between endothelial dysfunction and nitric oxide production in young male smokers. J Cardiol 2001; 38: 21–28 (in Japanese)
17) Falk E, Shah PK, Fuster V: Coronary plaque disruption. Circulation 1995; 92: 657–671
18) Liu W, Zhang Y, Yu CM, et al: Current understanding of coronary artery calcification. J Geriatr Cardiol 2015; 12: 668–675
19) Naoe S, Takahashi K, Masuda H, et al: Kawasaki disease with particular emphasis on arterial lesions. Acta Pathol Jpn 1991; 41: 785–797 (in Japanese)
20) Masuda H, Naoe S, Tanaka N: Pathology about coronary arteries associated with Kawasaki disease (MCLS)—Especially about the association between coronary arteritis and the morphogenesis of coronary aneurysms—. J Jpn Coll Angiol 1981; 21: 899–912 (in Japanese)
21) Takahashi K, Oharaseki T, Naoe S, et al: Neutrophilic involvement in the damage to coronary arteries in acute stage of Kawasaki disease. Pediatr Int 2005; 47: 305–310
22) Fujiwara T, Fujiwara H, Ueda T, et al: Comparison of macroscopic, postmortem, angiographic, and two-dimensional echocardiographic findings of coronary aneurysms in children with Kawasaki disease. Am J Cardiol 1986; 57: 761–764
23) Takahashi K, Oharaseki T, Naoe S: Pathological study of postcoronary arteritis in adolescents and young adults: With reference to the relationship between sequelae of Kawasaki disease and atherosclerosis. Pediatr Cardiol 2001; 22: 138–142
24) Cheung YF, Ho MH, Tam SC, et al: Increased high sensitivity C reactive protein concentrations and increased arterial stiffness in children with a history of Kawasaki disease. Heart 2004; 90: 1281–1285
25) Shioi A: Vascular calcification and remodeling in diabetes. J Jpn Coll Angiol 2010; 50: 561–567
26) Kobayashi T, Inoue Y, Otani T, et al: Risk stratification in the decision to include prednisolone with intravenous immunoglobulin in primary therapy of Kawasaki disease. Pediatr Infect Dis J 2009; 28: 498–502
27) Raaz-schrauder D, Klinghammer L, Baum C, et al: Association of systemic inflammation markers with the presence and extent of coronary artery calcification. Cytokine 2012; 57: 251–257
28) Weijis B, Blaauw Y, Rennenberg RJMW, et al: Patients using vitamin K antagonists show increased levels of coronary calcification: An observational study in low-risk atrial fibrillation patients. Eur Heart J 2011; 32: 2555–2562