Atrioventricular nodal reentrant tachycardia (AVNRT) is the second most common form of supraventricular tachycardia in children after atrioventricular reentrant tachycardia.1) The mechanisms underlying AVNRT episodes are classified into the common and uncommon types. Radiofrequency catheter ablation has been recommended for treatment of AVNRT. Both the common and uncommon types of AVNRT are treated by the ablation of the slow pathway. The success rate has been reported to be ≧95%.2, 3) However, it has been reported that the uncommon type includes numerous refractory cases and that it is associated with a high rate of relapse in comparison to the common type.4) Furthermore, few reports have so far examined the long-term outcomes after ablation treatment. In follow-up studies of adults after ablation for AVNRT, the reported rate of relapse at 5 years ranged from 0% to 7%.5–7) There are fewer reports on pediatric cases; such studies have reported rates of 4% to 9% at 1 year and 11% at 8 years.8, 9) We do not know of any pediatric reports describing a longer follow-up period.
In this study we aimed to elucidate the clinical features in pediatric patients with AVNRT who underwent ablation in our institute more than 15 years prior to the present study by asking them to respond to a questionnaire.
Study population
We aimed to survey 71 patients with AVNRT who underwent radiofrequency catheter ablation (RFCA) in our institute between May 1993 and September 2001 (total number of treatments, 90). The median age of the patients at the time of treatment was 14 years (range 1–39 years); 33 patients were male, and 38 were female. When the patients were treated before 20 years of age and had current contact information, questionnaire forms were mailed to either the patients or their family members for completion; they were returned by either a self-addressed envelope or facsimile transmission. We explained the precautions taken to protect personal information, the possible risks to the respondents, and the importance of the research in an information section of the questionnaire form. In addition to direct responses from the patient, we accepted questionnaires that were filled out by relatives or guardians. This research was conducted with approval from our hospital’s ethics committee (Ethics Committee Approval No. 27-205). The questionnaire focused on the patients’ perception of palpitations despite treatment by RFCA, whether or not medical evaluations were sought because of such symptoms, and the overall satisfaction with treatment (Table 1). In addition, the questionnaire survey revealed that many patients were aware of palpitations at the time of the survey. Thus, the subjects were divided into groups according to whether or not they recognized palpitations after RFCA (Group A, palpitations present; Group B, palpitations absent) in order to clarify the clinical features associated with palpitations from their medical records. We examined and compared following characteristics: the age when RFCA was performed, gender, body mass index (BMI), history of medication prior to the procedure (e.g., digoxin, verapamil, disopyramide, and cibenzoline), presence or absence of congenital heart disease, endpoint of RFCA, type of AVNRT, and repeat ablation.
Table 1 Questionnaire sent to patients| Questionnaire |
|---|
| Q1. Are you satisfied with the efficacy for treatment now? |
| □ Yes |
| □ No |
| Q2-A. For subjects who answered “Yes” to Q1: What is the reason? (Check all that apply.) |
| □ Not go to hospital regularly |
| □ Not restrict to exercise |
| □ Not feel uneasy |
| □ Not need to take medicine |
| □ Other (Please specify ) |
| Q2-B. For subjects who answered “No” to Q1: What is the reason? (Check all that apply.) |
| □ Recurrence |
| □ Complication |
| □ Repeat ablation treatment |
| □ Other (Please specify ) |
| Q3. Have you ever felt palpitations after catheter ablation? |
| □ Yes |
| □ No |
| Q4. For subjects who answered “Yes” to Q3: What is the reason? (Check one.) |
| □ Diagnosed with recurrence |
| □ Diagnosed with arrhythmia other than AVNRT ( ) |
| □ Went to hospital, received no diagnosis |
| □ Did not go to hospital |
| Q5. Would you like to tell us more in your own words? If so, please add any comments below. |
Electrophysiology Study (EPS) and the Ablation Protocol
Under intravenous anesthesia, all patients underwent fluoroscopically guided ablation treatment of the slow pathway. The catheter placement included a quadrupole in the high right atrium (HRA), a quadrupole in the His bundle, and a hexapole in the coronary sinus (CS) and right ventricle (RV). We administered isoproterenol when tachycardia was not induced. Until 1994 catheter ablations were performed for 40–60 s (determined by voltage: 40 V; current 300–600 mA) (RFG-3D, Radionics). Since 1995, ablation has been performed for 30–60 s (determined by temperature: 55–60°C) at a maximum of 40 W (HAT200, Osypka). Common AVNRT was diagnosed when the atrial site of earliest ventriculoatrial conduction activation during tachycardia was the anterior septal region; other patterns represented uncommon AVNRT. For the treatment of common AVNRT, the ablation site was determined by the anatomical information from the fluoroscopic image and/or the presence of Jackman’s potential. Meanwhile, the earliest atrial activation site during tachycardia was applied as the ablation site in patients with uncommon AVNRT. In patients with AVNRT that did not persist, the slow pathway region was ablated with reference to the fluoroscopic image. For both common and uncommon AVNRT, the success of RFCA was defined as one echo or the abolition of echo. Antiarrhythmic drugs were discontinued after ablation. The progress of the patients was evaluated, on an outpatient basis, for 5 years after the procedure.
Statistical Analysis
The EZR software program (Easy R Ver 1.31)10) was used to perform the statistical analyses. The age and BMI of the two groups was compared using the Mann–Whitney U test; Fisher’s exact test was used to compare all of the other variables. p values of <0.05 were considered to indicate statistically significant differences.
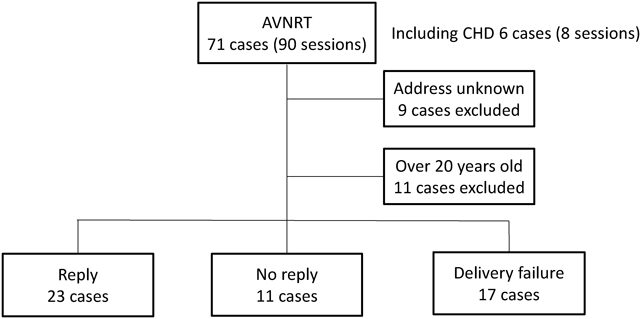
The Mailing and Return of the Questionnaires
Seventy-one patients with AVNRT underwent ablation (90 sessions) in our department (Fig. 1). We excluded 9 patients whose addresses were unknown and 11 who were ≧20 years of age at the time of ablation. The questionnaires failed to reach 17 of the remaining 51 patients because of a change of address. Eleven other potential subjects did not reply. Ultimately, 23 responses were received from the 51 patients (45%). The median time from the date of ablation to the date on which the questionnaire was 223 months (range 175–275 months).
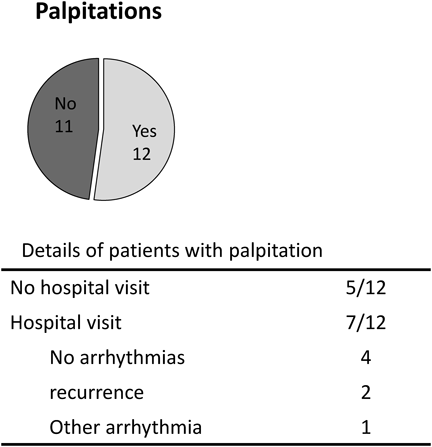
Replies to the Questionnaire
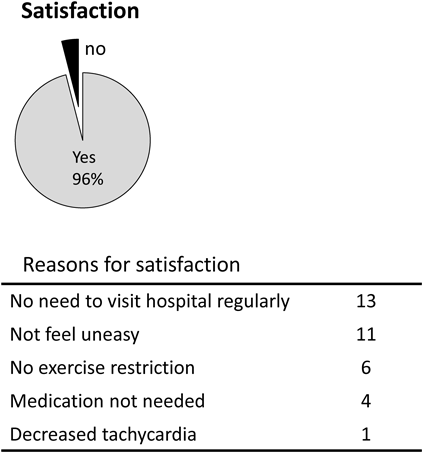
All respondents had sensations of palpitation prior to ablation. The results pertaining to palpitation after ablation are shown in Fig. 2. Twelve of the 23 respondents still sensed some palpitations after ablation (52%). Five of these twelve did not seek medical attention, while seven went to a hospital for evaluation. In 4, no arrhythmia was detected, and no diagnosis was made. Two of the 3 remaining subjects who sought evaluation were diagnosed with relapse; the other patient was diagnosed with a different arrhythmia. Due to the presence of these respondents, the long-term relapse rate of AVNRT after RFCA at our hospital was 9%. Fig. 3 shows the satisfaction with treatment. Twenty-two of the 23 respondents (96%) said that they were satisfied. With regard to the reasons for satisfaction, 13 respondents mentioned that they were satisfied because they did not need to regularly visit a hospital; 11 said that they no longer felt anxious—these responses were given by approximately half of the respondents. The next most popular responses were “no restriction of exercise” (n=6) and “no longer require medicine” (n=4)—these responses were given by approximately one-fourth of respondents. Only 1 subjects listed “decrease in tachycardia” under the other reasons.
Findings Associated with the Persistence or Absence of Palpitations (Table 2)
We did not identify any significant differences between the two groups in terms of age, gender, or BMI. The same was true for the satisfaction with treatment, which was reported by 11 respondents (92%) in Group A and 11 respondents (100%) in Group B. Hospital evaluation was sought by 7 respondents in Group A (58%) but none in Group B. Group A included 7 patients who were treated with medication prior to ablation (58%), while Group B included 1 such patient (9%). There was a significant difference (p<0.05). On the other hand, in regard to the presence or absence of congenital heart defects, the endpoint of RFCA, the type of AVNRT and repeat ablation, there were no significant differences between two groups. Two patients in Group A were diagnosed with relapse upon assessment at a hospital after the ablation.
Table 2 Comparison of patients with (A) and without (B) palpitations following ablation | Group A (n=12) | Group B (n=11) | p Value |
|---|
| Age in years (median, range) | 16 (9–19) | 13 (8–18) | 0.37 |
| Gender (M/F) | 3/9 | 4/7 | 0.67 |
| BMI (median, range) | 18.7 (14.2–21.5) | 22.2 (12.4–23.8) | 0.24 |
| Satisfaction (%) | 11 (96%) | 11 (100%) | 1 |
| Hospital evaluation | 7 (58%) | 0 (0%) | <0.05 |
| Medication | 7 (58%) | 1 (17%) | <0.05 |
| Slow/fast (%) | 8 (67%) | 10 (91%) | 0.32 |
| Echo abolished vs 1 echo persisting | 3 : 9 (25 : 75%) | 4 : 7 (36: 64%) | 0.67 |
| Repeat ablation | 3 (25%) | 1 (9%) | 0.59 |
| Congenital heart disease | 1 (8%) | 0 (0%) | 1 |
| BMI, body mass index; M, male; F, female. |
In the present survey, 96% of the respondents reported that they were satisfied with their treatment. We previously found that 98% of the respondents were satisfied after ablation treatment for Wolff-Parkinson-White (WPW) syndrome.11) Many AVNRT patients mentioned that they were satisfied with their treatment because they no longer needed to regularly visit a hospital; this was followed by reduced anxiety about attacks. The latter reason was also mentioned by our WPW syndrome patients. Prior to treatment, patients with WPW syndrome are typically warned about possible sudden death from untreated WPW syndrome. While anxiety has been reported to increase after the treatment of various reentrant tachycardias,12) our present respondents who were treated for AVNRT often cited their reduced anxiety about attacks as a reason for their satisfaction.
Even though 96% of our subjects were satisfied with their treatment, over half of our AVNRT patients still experienced some palpitations. This was higher than the proportion of patients who reported palpitations after ablation for WPW syndrome (28%).11) We were able to contact 5 of the 12 respondents who still had palpitations after RFCA by telephone. Among these subjects, 3 considered the palpitations to be the same sort that they had experienced before ablation, while the remaining 2 reported that the continuing palpitations were considered to be premature beats. Overall, we considered the persistence of palpitations to be a useful indication for an electrophysiological study to investigate the possible relapse of AVNRT, and—if indicated—to perform retreated.
In our survey, the long-term relapse rate in patients with AVNRT was higher than that of WPW syndrome we reported before (9% vs 0.5%).11) While the relapse of WPW syndrome can be diagnosed by identifying a delta wave on an electrocardiogram (ECG), patients with AVNRT show normal ECG findings, except when they experience a clinical attack. All the more reason, it is important to pay attention to a clinical symptom even after a successful RFCA.
We divided subjects into two groups according to whether or not they recognized palpitations after RFCA and compared their clinical features. A significant difference was found between two groups in the medications taken prior to the ablation. Seven of the patients in Group A took some medicines. In three of them, the reason why they take medication was anxiety which may have a tachycardia attack again. Among them, two took verapamil only when they have a tachycardia attack. One patient who had a premature ventricular contraction (PVC) as a comorbidity required medication for PVC. One patient took digoxin although we do not know the reason. The remaining three patients were complicated cases. One patient was diagnosed to have ventricular septal defect (VSD) and underwent tricuspid valve replacement after VSD closure. The remaining two patients were uncommon AVNRT. In other words, the patients who complain of palpitations after RFCA were more likely to have anxiety before RFCA and complicated case. In this study, many patients have reported their palpitations after long passage as 15 years. Although our hospital has finished regular follow-up in 5 years after RFCA, we have to create a system such as the patients can be re-examined long after the RFCA.
Limitations
In this study, we demonstrated the long-term clinical features of AVNRT after RFCA. However, there were some limitations. First, this study is based on a questionnaire survey and investigates the clinical features of the remote period. Therefore, long-term results after RFCA cannot be mentioned. Second, since less than half of the subjects responded to the questionnaires, the answers might not have been representative of the larger group. Third, many patients who reported palpitations did not undergo ECG assessments, which leaves open the possibility that our analysis might have missed some subjects with relapse. When possible, we sought to increase our accuracy with respect to this issue by conducting telephone interviews with the subjects who experienced palpitations.
Although more than half of the AVNRT patients in the present study still were aware of palpitations after ablation, many patients were satisfied with the treatment. Even though the causes of continued palpitations were often not elucidated, some relationship existed between persistent palpitations and a history of anti-arrhythmic medication prior to ablation. In patients with AVNRT, relapse should be suspected when palpitations recur or persist, and electrophysiological studies should be performed when necessary.
Conflict of Interests
The authors have no conflict of interest to disclose.
引用文献References
1) Anand RG, Rosenthal GL, Van Hare GF, et al: Is the mechanism of supraventricular tachycardia in pediatrics influenced by age, gender or ethnicity? Congenit Heart Dis 2009; 4: 464–468
2) Krause U, Backhoff D, Klehs S, et al: Catheter abalation of pediatric AV nodal reentrant tachycardia: Results in small children. Clin Res Cardiol 2015; 104: 990–997
3) Yaminisharif A, Davoodi G, Kasemisaeid A, et al: Radiofrequency catheter ablation of atrioventricular nodal reentrant tachycardia: Success rates and compalications during 14 years of experience. J Tehran Univ Heart Cent 2010; 5: 87–91
4) Feldman A, Voskoboinik A, Kumar S, et al: Predictors of acute and long-term success of slow pathway ablation for atrioventricular nodal reentrant tachycardia: A single center series of 1,419 consecutive patients. Pacing Clin Electrophysiol 2011; 34: 927–933
5) Kimman GP, Bogaard MD, van Hemel NM, et al: Ten year follow-up after radiofrequency catheter ablation for atrioventricular nodal reentrant tachycardia in the early days forever cured, or a source for new arrhythmias? Pacing Clin Electrophysiol 2005; 28: 1302–1309
6) Clague JR, Dagres N, Kottkamp H, et al: Targeting the slow pathway for atrioventricular nodal reentrant tachycardia: Initial results and long-term follow-up in 379 consecutive patients. Eur Heart J 2001; 22: 82–88
7) Femenía F, Arce M, Arrieta M, et al: Long-term results of slow pathway ablation in patients with atrioventricular nodal reentrant tachycardia: Simple approach. J Electrocardiol 2012; 45: 203–208
8) Kubuš P, Vít P, Gebauer RA, et al: Long-term results of paediatric radiofrequency catheter ablation: A population-based study. Europace 2014; 16: 1808–1813
9) Backhoff D, Klehs S, Müller MJ, et al: Long-term follow-up after catheter ablation of atrioventricular nodal reentrant tachycardia in children. Circ Arrhythm Electrophysiol 2016; 9: e004264
10) Kanda Y: Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48: 452–458
11) Aoki H, Nakamura Y, Fukuhara H, et al: Long-term follow-up results after percutaneous radiofrequency catheter ablation in children with WPW syndrome. J Jpn Soc Pediatric Cardiol Card Surg 2013; 29: 331–338
12) Schlapfer J, Fromer M: Late clinical outcome after successful radiofrequency catheter ablation of accessory pathways. Eur Heart J 2001; 22: 605–609