The patient was a 15-year-old girl. She had visited our hospital for thrombocytopenia at 13 years of age. The blood examination resulted in a decrease in complement and an anti-nuclear antibody (anti ds-DNA antibody) being positive. And she became a diagnosis of SLE. At that time, we performed echocardiography as the routine examination for SLE. Echocardiography showed hypoplasia of the right ventricle, no abnormality was found in the attachment position and morphology of the tricuspid and pulmonary valve. And the tricuspid valve annular diameter and pulmonary valve annular diameter were also normal.
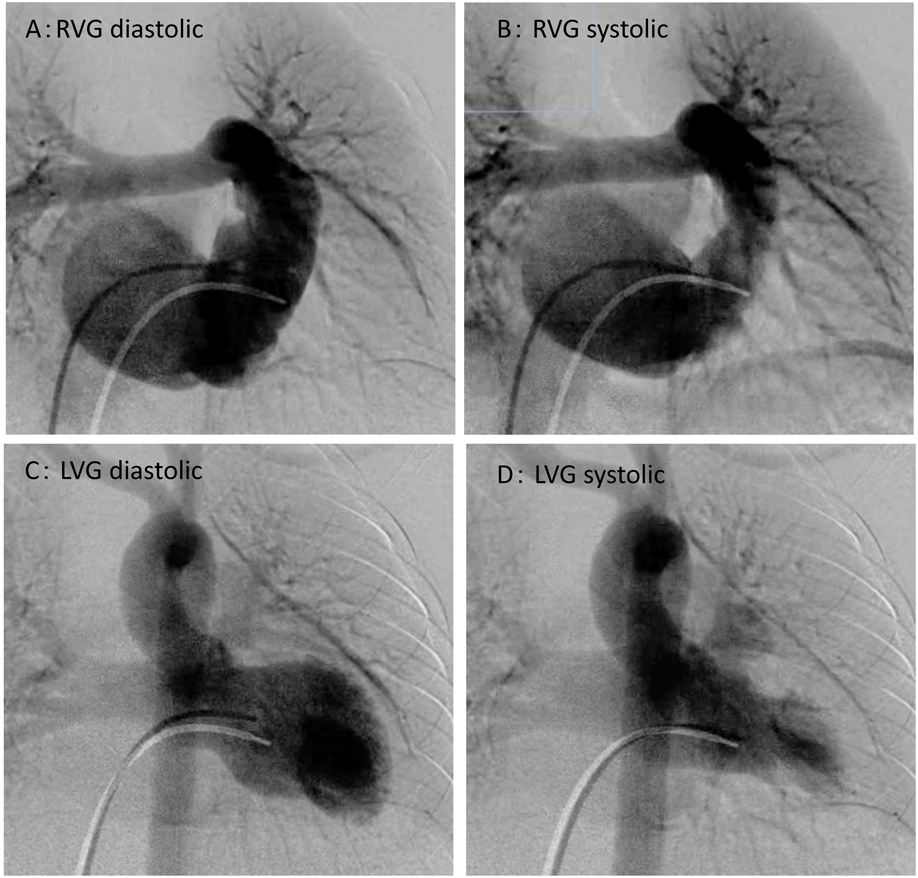
In addition, cardiac catheterization and angiocardiography were performed to examine her heart in detail (Fig. 1, Table 1).
Table 1 Cardiac catherization| Site | 13 years | 15 years |
|---|
| Pressure mmHg Systolic/diastolic (mmHg) | Oxygen Saturation (%) | Angiography | Pressure Systolic/diastolic (mmHg) | Oxygen Saturation (%) | Angiography EDV (mL) |
|---|
| SVC | 10/5 (mean 6) | 58.0 | | 14/6 (mean 6) | 58.4 | |
| RA | 13/6 (mean 6) | | | 14/5 (mean 6) | | |
| RV | 13/edp 6 | | | 12/edp 10 | | |
| EDV (%of Normal) | | | 45 mL (58) | | | 54 mL (60) |
| ESV (%of Normal) | | | 21.1 mL (51) | | | 20.0 mL (57) |
| SV | | | 24 mL | | | 33 mL |
| EF | | | 53% | | | 63% |
| mPA | 13/4 (mean 5) | 64.6 | | 12/4 (mean 5) | 61.5 | |
| Ao | 110/63 (mean 78) | 99.4 | | 90/55 (mean 70) | 98.8 | |
| LV | | | | 90/edp 4 | | |
| EDV (%of Normal) | | | 77 mL (99) | | | 58 mL (65) |
| ESV (%of Normal) | | | 25.1 mL (93) | | | 13.9 mL (41) |
| EF | | | 65% | | | 76.2% |
| Qp/Qs | | 1.0 | | | 1.0 | |
| C.I. | | 2.1 | | | 1.7 | |
| Ao; aorta, C.I.; cardiac index, edp; end-diastolic pressure, EDVI; end-diastolic volume index, EF; ejection fraction, ESVI; end-systolic volume index, LV; left ventricle, mPA; mein pulmonary artery, RA; right atrium, RV; right ventricle, SVC; supra vena cava, SVI; stroke volume index. |
Right ventriculography showed hypoplasia with an end-diastolic right ventricular volume of 45 mL (58% of normal). The diagnosis was isolated hypoplasia of the bipartite right ventricle, which did not affect the muscle. Although we were not able to confirm the shunt between the right and left atrium, the left ventricular end-diastolic volume was 77 mL (99% of normal), and the ejection fraction was 65%.
At 15-years of age, she complained of exertional dyspnea and her BNP level rose to 700 pg/mL (BNP at 13-years was 200 pg/mL.). She was therefore hospitalized and treated with intravenous diuretics. However, her heart failure subsequently recurred whenever she had a common cold. We started medical treatment with an anti-pulmonary hypertension drug(Ambrisentan) and β blocker(Carvedilol). She was hospitalized again because her symptoms showed no improvement.
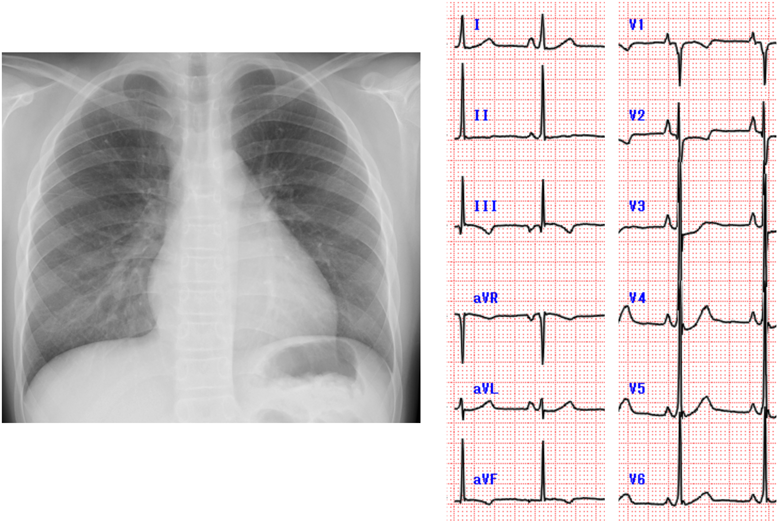
On a chest X-rays, the CTR was 51%, and the pulmonary vascular shadow was normal. Electrocardiogram showed right atrium enlargement (Fig. 2).
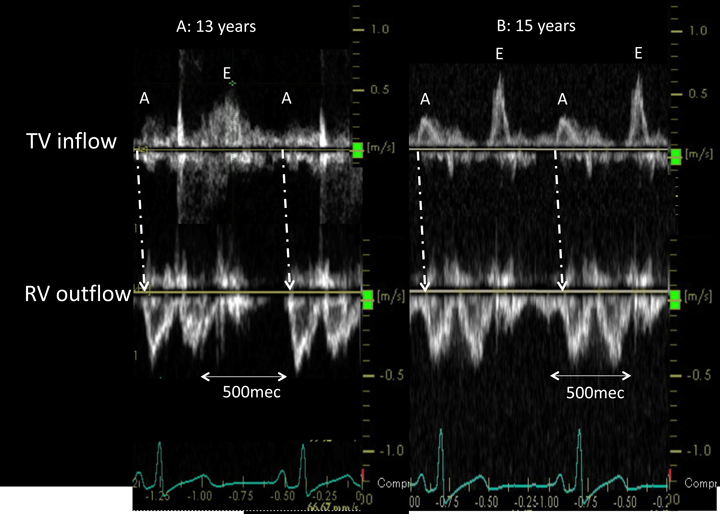
Echocardiography showed paradoxical movement of the interventricular septum in the long axis view and hypoplasia of the right ventricle in the four-chamber view. There was no shunt between the right and left atrium. Left ventricle was the compaction, and trabeculation of right ventricle was the coarse. Doppler echocardiography showed biphasic anterograde pulmonary flow (Fig. 3). One phase involved anterograde flow due to right ventricular contraction. The other involved end-diastolic forward flow to the pulmonary artery, which was consistent with the A wave of atrial contraction.
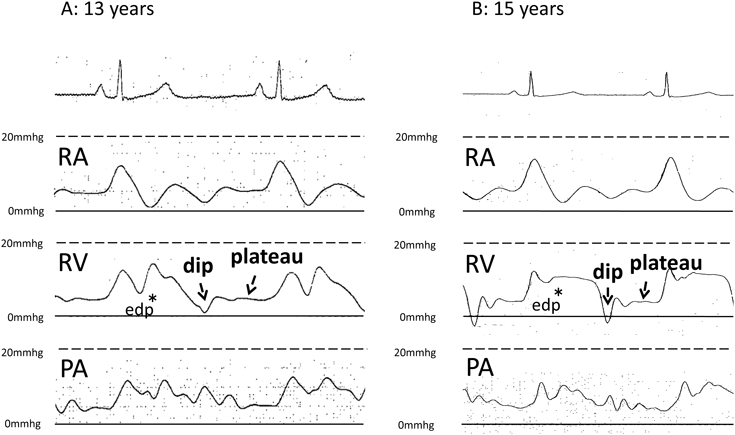
In the waveform of the right ventricular inflow portion, the interval between the E wave and the A wave was flat, and the diastolic disorder of the right ventricle was suspected. Fig. 4 shows the pressure wave form of the cardiac catheterization. The increases in the pulmonary arterial pressure and right ventricular pressure were consistent with an increase in atrial pressure with the atrial A wave. The pulmonary artery pressure increased as the right ventricular pressure increased at 13 years of age. However, when cardiac catheterization was performed at 15 years of age, the increase in the right ventricular end-diastolic pressure. Moreover, the waveform of this right ventricle clearly showed a dip and plateau. We thought that the restrictive myocardial myopathy had worsened.
The comparison of the cardiac catheterization findings obtained at 15 and 13 years of age, revealed that the right ventricular end-diastolic volume was the same (54 mL; 60% of normal), while the left ventricular end-diastolic volume was clearly decreased (58 mL; 65% of normal). The cardiac index had decreased to 1.7. However, there was no decrease in the right ventricular stroke volume from 24 to 33 mL and contraction rate from 53 to 63%. From those results, it was determined that right ventricle was disfunction, and it was a limit in medical treatment. Therefore we decided to use Fontan procedure in order to supply left ventricular volume in this case.
The clinical symptoms of isolated right ventricular hypoplasia vary according to the size of the right ventricle and the intraatrial shunt, and it is said that cases with large atrial septal defects may pass until adulthood without symptoms.2)
No heart symptoms (including cyanosis) were pointed out until the patient was examined for SLE at 13 years of age. She did not have cyanosis at the consultation, and no intraarterial shunt was found. Ventriculography revealed right ventricular end-diastolic hypoplasia (volume 58% of normal), while the left ventricular end-diastolic volume was normal (98% of normal). Because right to left shunt at the intraatrial level compensates for the pre-loading of the left ventricle, the left ventricular volume remains normal in this disease. However, the left ventricular volume was normal despite the patient not having right to left shunt at the intraatrial level. Cardiac catheterization did not show any other shunt that would cause left ventricular pre-loading.
Echocardiography showed forward diastolic flow to the pulmonary artery coincident with atrial contraction. It was anterior blood flow due to the atrial contraction during the end-diastolic phase. We think that this anterior blood flow due to atrial contraction maintained a normal left ventricular volume without intraatrial shunt. Similar end-diastolic forward flow to the pulmonary artery is reported in intermediate postoperative tetralogy of Fallot.3) This end-diastolic forward flow suggested restrictive physiology of the right ventricle. Thus, we think that this end-diastolic forward flow made up for insufficient right ventricle cardiac output due to the restrictive physiology of the right ventricular myocardium.
Palliative surgery such as Glenn surgery and atrial septal closure are selected for the treatment of this disease; it has been proposed that the surgical procedure should be selected after closing the defect using a balloon catheter.4) However, there are reports of the occurrence of arrhythmia and deterioration of the cardiac function within 11 years after atrial septum closure operations.5) Abnormality of the right ventricular myocardium is pointed out as cardiac dysfunction much later in life, and it is suggested that this disease may change not only the volume of the right ventricle of this disease but also the properties of the myocardium.
Similarly, the possibility of a right ventricle myocardial anomaly was considered in the present case. At 15 years of age, the patient’s left ventricular end diastolic volume had obviously decreased to 65% of the normal value, and the cardiac index had also decreased to 1.7. Although the pulmonary blood flow detected by echocardiography was biphasic, as had been observed in the past, the right ventricular pressure wave-form showed a clear dip-and-plateau and an increase diastolic pressure. In other words, we think that the right ventricular restrictive change had progressed.
Due to the progression of the right ventricular restrictive change, a high atrial contraction pressure was required for auricular contraction to generate pulmonary blood flow. In fact, the magnitude of the A wave at age 15 was smaller than at age 13 (Fig. 3).
For this reason, a higher atrial contraction pressure was required to maintain the pulmonary blood was flow by atrial contraction, blood was sent to the right ventricle at diastole when the right atrial level decreased, and conversely the reverse blood flow into the vena cava system increased.
Thus, when considering the treatment strategy for isolated right ventricular hypoplasia, it is necessary to determine the right ventricular volume and to keep the possibility of restrictive change in mind.