Tuberous sclerosis complex (TSC) is a genetic disease associated with mutation of the TSC gene, which contributes to abnormal tumor suppression activity. Patients with TSC often have mass lesions in various organs, including the brain, heart, lungs, and kidneys. In particular, among infants, TSC is often diagnosed according to the presence of a congenital cardiac tumor, which is the leading complication. A primary cardiac tumor is rare in infants and children, and approximately 70% of tumors are rhabdomyomas.1) With regard to the rhabdomyoma tumor type, most cases involve tuberous sclerosis, and this tumor type has been adopted as one of the diagnostic criteria for tuberous sclerosis. Delmo Walter et al. reported congestive heart failure in 2 of 47 children with cardiac tumors (4.2%).1) Everolimus, an inhibitor of mammalian target of rapamycin (mTOR), has been approved for use in the treatment of renal angiomyolipoma and subependymal giant cell astrocytoma (SEGA). However, it is not approved for use in the treatment of cardiac tumors, although there are some reports on the effectiveness of everolimus for cardiac tumors.2–10) Here, we present the case of a patient with heart failure who was diagnosed with a large cardiac tumor as a neonate and was successfully treated with everolimus. The outcome of this case suggests that everolimus treatment started at an early age is very effective in the treatment of cardiac tumors.
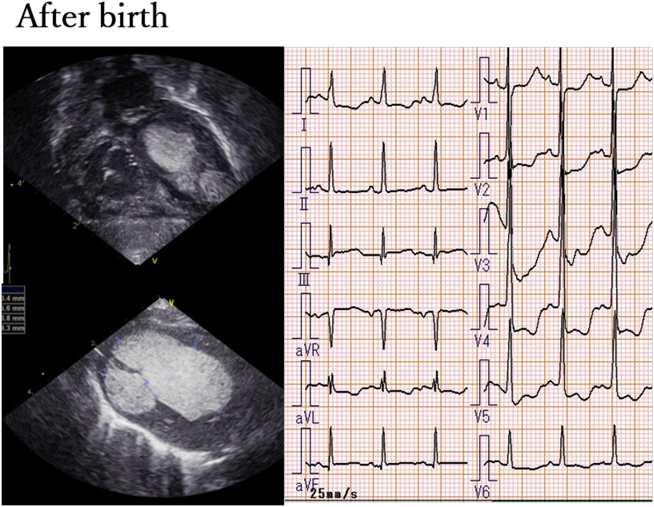
A female child was born at 39 weeks to a 27-year-old woman without any relevant family history. She was the first child of an unrelated healthy couple. Neither her parents nor relatives had tuberous sclerosis. Screening at 25 weeks of gestation using ultrasonography revealed a cardiac tumor, and she was referred to our hospital at 28 weeks of gestation. At 34 weeks of gestation, magnetic resonance imaging revealed TSC as a definitive diagnosis, with multiple nodules around the lateral ventricles and cardiac rhabdomyomas. There were multiple heart rhabdomyomas, and in particular, a large tumor occupied the left ventricle. Because of concerns regarding circulation after birth, delivery was planned at 39 weeks of gestation. Her parents were informed that the tumor was considerably large for her to survive without early surgery and that everolimus might help avoid or delay surgery. Her parents requested for the use of everolimus at birth, and permission was granted by the TSC board and the Ethics Committee of Juntendo University (approval No.: 16-0027). We planned to use everolimus for survival in case of heart failure. At 39 weeks of gestation, she was born via normal vaginal delivery. Her Apgar scores at 1 and 5 min were 9 and 9, respectively. Her birth weight was 2,844 g, heart rate was 116 beats/min, blood pressure was 65/32 mmHg, and oxygen saturation was 95% with room air. Physical examination revealed mild cyanosis and mild hepatomegaly. We noted a grade 2–3/6 systolic ejection murmur, which was best heard at the left sternal border. Transthoracic echocardiography demonstrated multifocal echogenic masses. There were 2 masses in most of the left ventricle (apex to outflow; 30.4×15.6 mm at the interventricular septum side and 13.8×8.3 mm at the posterior wall side), resulting in mild outflow obstruction; 3 masses at the right ventricular apex and inflow and outflow tracts (12.6×8.4 mm, 5.0×6.0 mm, and 4.7×2.7 mm, respectively); and 1 mass at the right atrial appendage (4.5×5.4 mm). The left ventricular ejection fraction could not be measured by M-mode echocardiography because of the large left ventricular mass. The blood flow of the left and right ventricular inflow and outflow tracts was smooth. The flow rates of the left and right ventricular outflow tracts were 1.08 and 0.98 m/s, respectively. In a parasternal 4-chamber view, there was no dilatation of the atrium or ventricle. The estimated right ventricular pressure was almost equal to the left ventricular pressure. A small foramen ovale with left-to-right shunting and ductus arteriosus with bidirectional shunting were detected.
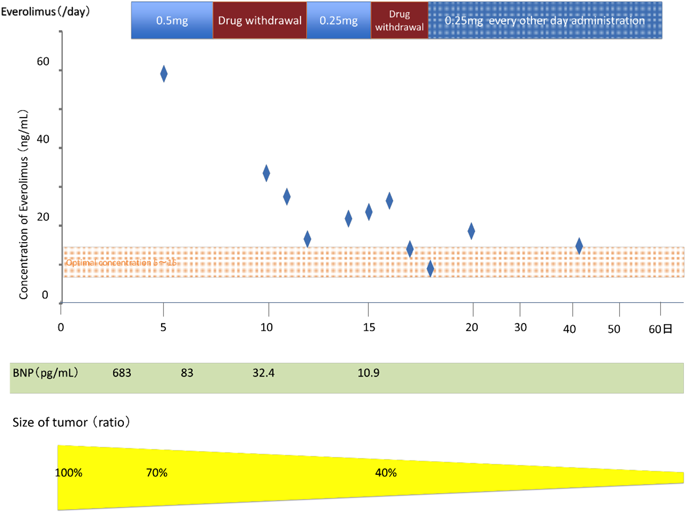
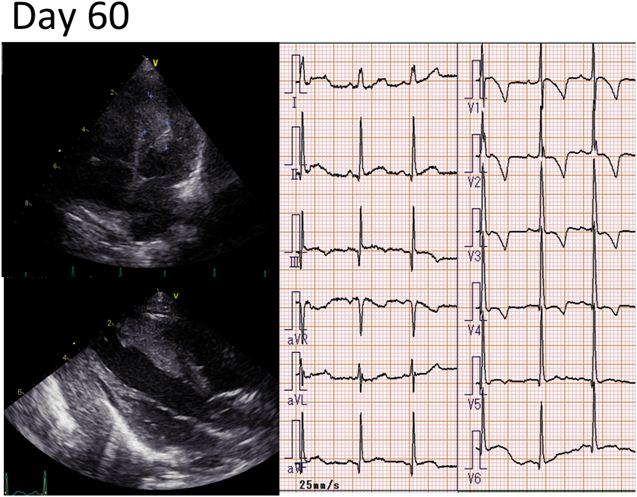
The SpO2 level marginally decreased (95%), and the heart rate and blood pressure were maintained at 136 beats/min and 65/32 mmHg, respectively. The tendency of hyperventilation (50 times/min) was mild, but retraction was noted. The stroke volume of the left ventricle was anticipated to be small because of an occupational lesion in the heart. Additionally, the patent ductus arteriosus was bidirectionally shunting even after 24 h from birth. Thus, transductus arteriosus blood flow was possibly necessary for the maintenance of systemic circulation. Accordingly, we decided to administer prostaglandin E1 (0.01 µg/kg/min). On resting electrocardiography, a low ST level at V2 and a negative T wave at V3–V6 were detected. QTc was 410 ms (Fig. 1). At 3 days of age, everolimus treatment at a dose of 3 mg/m2 (0.5 mg) once daily was started, according to the generally recommended dose.11) Her whole blood cell count, hepatic and renal function levels, and electrolyte and serum everolimus levels were monitored. At 6 days of age, echocardiography showed a smaller cardiac tumor and ductus arteriosus with a left-to-right shunt; thus, prostaglandin E1 was discontinued. At the same time, the first serum everolimus trough level was 59 ng/mL, and the treatment was suspended at 8 days of age. We found that the ductus arteriosus and foramen ovale had closed at 8 days of age. At 12 days of age, the serum everolimus level was 16 ng/mL, and everolimus treatment was restarted on the next day at 1.5 mg/m2. At 14 days of age, the serum everolimus level was 21.8 ng/mL; thus, treatment was skipped on the next day and was restarted at 16 days of age at 1.5 mg/m2 every other day. After changing the dose, the serum everolimus level remained in the therapeutic range (5–15 ng/mL) (Fig. 2). At 28 days of age (25 days after everolimus treatment was started), echocardiography showed that the right and left ventricle cardiac tumors were approximately one-quarter of their previous sizes. Additionally, there was no obstruction of the inflow and outflow tracts. At 31 days of age, she was discharged from the hospital (Fig. 3). During hospitalization, diaper dermatitis was detected, but it was unclear whether it was related to everolimus. Leukocytosis and thrombocytosis were identified as adverse events, and everolimus treatment was completed at 72 days of age. At discontinuation, her WBC count was 17,800/µL (36% neutrophils, 6.5% monocytes, 14% eosinophils, and 0.5% basophils) and platelet count was 86.8×104/µL. Subsequently, the symptoms of leukocytosis and thrombocytosis improved. At 5 months and 17 days of age, the tumors in the left ventricle showed slight enlargement (10.0×5.0 mm at the ventricular septum side and 9.0×6.0 mm at the posterior wall side); however, the increase was not progressive. This case has been followed up since over 2 years now, and no intracardiac obstructions or symptoms of heart failure have been noted.
TSC is a neurocutaneous syndrome that causes hamartomas in systemic organs. It is an autosomal dominant disease, but two-thirds of cases involve mutations. The causative gene is the TSC1 or TSC2 gene. There is suppression of mTOR signal transduction, which is related to cell segmentation and angiogenesis. In TSC, the tumor suppression mechanism decreases, whereas the activity of mTOR increases. Increased cell multiplication causes tumors in systemic organs.12) Everolimus, a rapamycin derivative, is an oral mTOR inhibitor. The effects of everolimus treatment on SEGA and renal angiomyolipoma have been demonstrated. Recent studies have suggested that everolimus is effective against cardiac tumors in cases of TSC.4–12) In our case, the tumors caused low cardiac output and ductus arteriosus-dependent circulation. The tumors quickly decreased in size after the initiation of everolimus treatment, and heart failure improved after 3 days of treatment. After 3 months of treatment, the tumors decreased to acceptable sizes. After treatment discontinuation, there was a slight increase in the tumor size, but it was not progressive. The control of the serum everolimus level was difficult. There is no standard protocol for the use of everolimus in cases of cardiac rhabdomyomas. In cases of SEGA with TSC, the protocol is 3 mg/m2 once/day, with the serum level maintained at 5–15 ng/mL. For cardiac rhabdomyomas, a previous study used a dose of approximately 3 mg/m2; hence, approval was obtained from the Ethics Committee, as obtained by the previous study group.11) However, owing to the limited description of blood levels, we decided to adjust the trough blood level to 5–15 ng/mL. Additionally, we obtained approval from the Ethics Committee when the cardiac tumors reduced or when side effects occurred, and the administration was subsequently discontinued. We followed the protocol, but the serum levels were very high. Accordingly, the dose was reduced, and the serum level stabilized within the therapeutic range at a dose of 1.5 mg/m2 every other day. There is a possibility that the serum everolimus level in neonates can be maintained within the therapeutic range with a lower dose than that reported previously.4–12) Our case involved heart failure; thus, there was intestinal ischemia and hepatic congestion. As everolimus is metabolized in the liver and intestinal tract and combined with albumin, each case might need dose adjustment. Further reports are needed on the use of everolimus treatment for cardiac rhabdomyomas.
In our case, there were no complications, such as interstitial pneumonia and mucositis, suggesting that everolimus treatment is safe when used in neonates. Krueger et al. reported that the mechanism of TOR signal suppression is related to brain development and function; thus, everolimus use in neonates should be as minimal as possible.13) There is no standard treatment period, but everolimus has been administered for almost 3 months in most cases. In our case, the tumor size reduced, heart failure improved, and feeding or weight gain difficulty was not noted with treatment, and the treatment was completed in 3 months.
Bornaun et al. reported that cardiac tumors became larger after discontinuation of everolimus treatment and treatment was restarted.2) In our case as well as this report, the tumors became larger, but were not progressive, and heart failure did not reoccur. It is important to carefully monitor tumor size after completing everolimus treatment.
Nield et al. identified 130 children with primary pediatric intracardiac tumors. Of these children, 14 (11%) had outflow obstruction based on a peak-pulsed Doppler outflow gradient >20 mmHg. Additionally, 36 children (28%) presented with at least 1 intracardiac tumor extending into the right or left ventricular outflow tract, and 12 of these children (33%) required surgery.14) It is expected that everolimus treatment will make it possible to non-invasively treat cardiac rhabdomyomas most often seen in cases of pediatric cardiac tumors.