A right aortic arch with aberrant left innominate artery is a rare form of vascular ring. To date in the literature, only 10 reports or so documented this circumstance.1, 2) Furthermore, to the best of our knowledge, there have been no published reports on a successful surgical approach in an extremely low-birth weight infant with this abnormality.
Here, we report a case of successful transection of the left-sided patent ductus arteriosus (PDA) to treat a complete vascular ring in such a small infant. Written informed consent for publication was obtained from the parents.
The patient was a 32-day-old girl weighing 0.9 kg. She was urgently delivered via the cesarean section at 34 weeks of gestation, weighing 788 g, at another hospital. She was immediately intubated due to respiratory failure. Upon investigating her up, the echocardiographic screening revealed a large PDA, resulting in a reversed diastolic flow through the descending aorta. Clinically, her symptoms of heart failure gradually deteriorated. Indomethacin was administered twice on hospital days 10 and 11. Despite the medical therapy, the patient’s symptoms related to PDA (including those probably attributed to renal dysfunction) were getting worse. On hospital day 21, she was transferred to our hospital for further management.
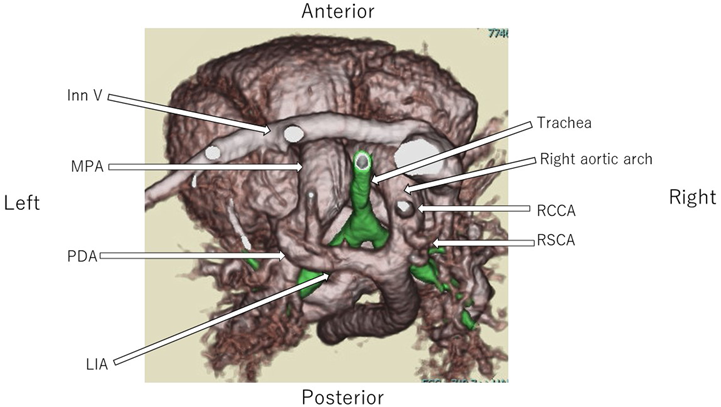
During our preliminary physical examination of the patient, a bounding pulse was palpated and a continuous murmur was audible. The large PDA was reconfirmed on echocardiography, but this imaging modality was unable to illustrate the full extent and course of the PDA due to its tortuosity. Additionally, we suspected that her neck vessel branches were anatomically abnormal. Upon further evaluation, computed tomography angiography (CTA) of the chest with a three-dimensional reconstruction revealed the following: (1) a right aortic arch, and (2) the third (last) arterial branch originating from the descending aorta with the left-sided PDA connected to the pulmonary artery (Fig. 1). The third arterial branch was determined to be the aberrant left innominate artery. This aortic arch malformation formed a complete vascular ring, which compressed the trachea.
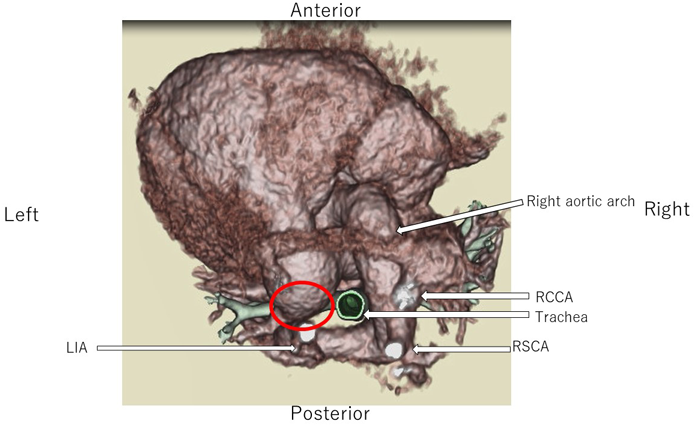
In general, clipping is a typical procedure in premature infants with PDA. In our particular patient, we decided to choose transection of the left-sided PDA via a thoracotomy for immediate decompression of the trachea. During the operation, at first, the right aortic arch and the left innominate artery coursing behind the esophagus were identified. Subsequently, we located the PDA which bridged from the left innominate artery to the pulmonary artery. Eventually, the PDA was divided to interrupt the vascular ring. After surgery, the patient was successfully extubated. The postoperative course was uneventful. Postoperative CTA confirmed that her vascular ring had been relieved (Fig. 2).
Vascular ring is a malformation of the aortic arch wherein the trachea and the esophagus are completely surrounded by vascular structures. The common form is double aortic arch, or right aortic arch with an aberrant left subclavian artery from the diverticulum of Kommerell. The arch abnormality seen in this patient, a right aortic arch with aberrant left innominate artery and left-sided patent ductus arteriosus, is rare. The earliest report of such an example is dated back in 1968.3) Since then, the abnormality has been reported either in isolation4) or in conjunction with other congenital cardiac malformations.5) As for surgical treatment, there have been no reports of successful repair in extremely low-birth weight infants. Our report is the first to document a successful surgical approach in this setting.
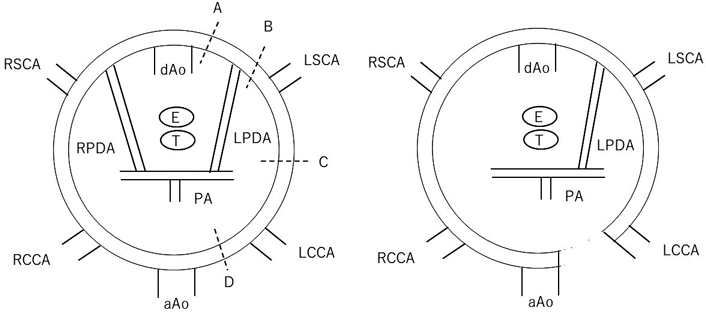
The variation of right aortic arch with aberrant left innominate artery arising from the descending aorta was originally explained by the Edwards’ hypothetical model of double aortic arch.2) When the right aortic arch is persistent, there are four patterns in interruption or remnants of the left aortic arch, the latter being designated as the left innominate artery.6) Figure 3 illustrates the major vessels of the vascular ring with a right aortic arch and a right-sided descending aorta.7) Anomalous interruption of the left aortic arch can occur in any of the four positions (A–D). If interrupted at A or B, the remnant of the left aortic arch remains as the Kommerell’s diverticulum (the most common abnormality),8) whereas an interruption at D, as in this case, is especially rare. The latter results from an interruption of the left aortic arch between the ascending aorta and the left carotid artery during embryonic vascular development.9) In this abnormality, the aortic arch lies on the right side of the trachea. The first, the second, and the third branches become the right common carotid, the right subclavian, and the left innominate arteries, respectively. The aberrant left innominate artery arises from the distal aortic arch, passes behind the esophagus, and serves as the origin of the left carotid and the subclavian arteries.10, 11) This abnormality produces a vascular ring, which causes a tracheoesophageal compression. The vascular ring is composed of the right arch on the right side, the left innominate artery at the back, and the pulmonary artery in front. The PDA or ligamentum arteriosum completes the ring on the left side by connecting the left innominate artery to the left pulmonary artery.
Transection of the PDA is appropriate when the structure forms a vascular ring, rather than usual clipping carried out to treat premature PDA. In such a circumstance, it is pertinent to follow the entire course of the PDA. Since the echocardiography was unable to reveal the whole PDA and the neck vessel branches, CTA was performed to confirm the presence of a vascular ring. This investigation identified the anatomical feature of the vascular malformation in our patient, which was helpful in formulating the definitive strategy and management plan. Furthermore, PDA transection appeared particularly sensible even when the PDA was small, since the risk of compression onto the trachea and the esophagus would be imminent in the future. We re-emphasize that accurate and complete diagnosis of the PDA using CTA is important in the vascular ring variety, and that the PDA can be divided without any complications even in an extremely low-birth weight infant.
 1,Takuya Fujisaki1,Masayoshi Mori1,Yoichiro Ishii1,Hisaaki Aoki1,Kunihiko Takahashi1,Shigemitsu Iwai2,Futoshi Kayatani1Kumiyo Matsuo1, Dai Asada
1,Takuya Fujisaki1,Masayoshi Mori1,Yoichiro Ishii1,Hisaaki Aoki1,Kunihiko Takahashi1,Shigemitsu Iwai2,Futoshi Kayatani1Kumiyo Matsuo1, Dai Asada