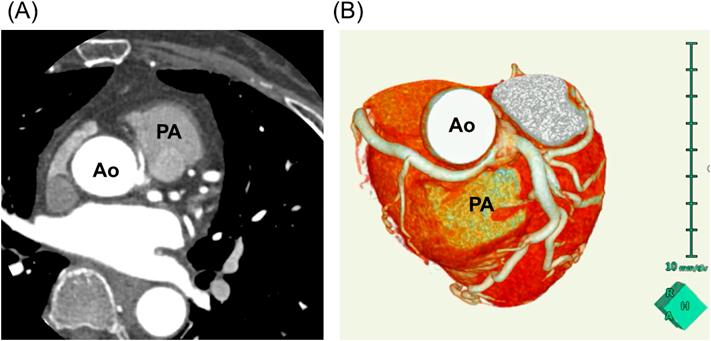
A 65-year-old woman with a history of exercise-related angina was referred to our hospital. She had no history of syncope or ventricular arrhythmia, and no coronary risk factors. The electrocardiogram at rest was within normal limits, and echocardiogram showed no left ventricular asynergy. However, laboratory data indicated elevated troponin I (74.5 pg/mL). She underwent coronary angiography, which revealed AAORCA. Coronary 3D computed tomography (CT) showed the RCA departing independently from the left coronary sinus of Valsalva and passing between the ascending aorta and the pulmonary trunk (the so-called interarterial course) (Fig. 1A, B).
Myocardial perfusion scintigraphy failed to exhibit ischemia; nonetheless, electrocardiogram exercise testing revealed ST depression in leads II, III, and aVF. Thus, we recommended surgical intervention based on the guideline.2)
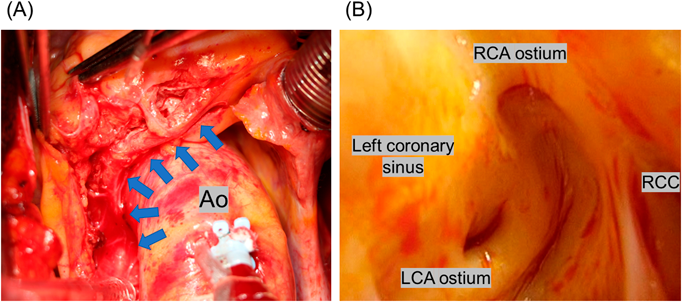
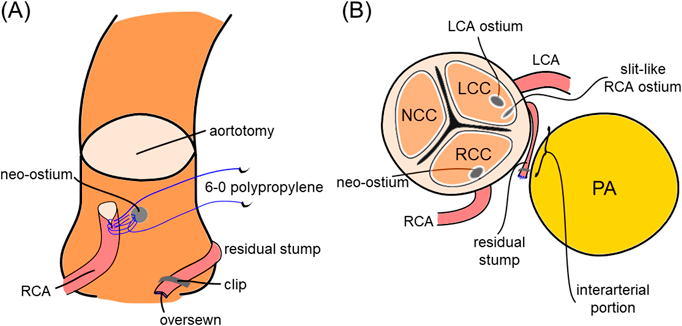
Through a median sternotomy, the AAORCA was identified (Fig. 2A); using a harmonic scalpel, we dissected the proximal portion of the RCA just distal to the intramural portion for 2 cm, sparing the proximal branches. The superior aspect of the RCA was marked to prevent distortion. Cardiopulmonary bypass was established by cannulation to the ascending aorta and the right atrium. The left ventricular venting tube was inserted via the right upper pulmonary vein. The initial cardioplegia was infused antegradely from the aortic root. A transverse aortotomy was performed 15 mm above the sino-tubular junction. We confirmed that both the left coronary artery and the RCA originated independently from the left coronary sinus of Valsalva, and that the RCA ostium was slit-like (Fig. 2B). We transected the RCA adjacent to the intramural portion. The residual proximal stump was 10 mm long. The stump was clipped, and the amputated end was oversewn with 7-0 polypropylene. The wall of the very proximal ascending aorta, just above the sino-tubular junction on the right facing sinus aspect, was punched out to create a neo-ostium. The RCA was spatulated for 4 mm on the inferior side and was anastomosed to the neo-ostium using running 6-0 polypropylene beginning at the heel. The aortotomy was closed in two layers. After infusion of warm cardioplegia, the aorta was unclamped. Electrocardiogram showed normal sinus rhythm with no significant ST-T change. The RCA flow was measured intraoperatively as 54 mL/min using doppler ultrasound. A schematic illustration of the surgery is shown in Fig. 3A, B.
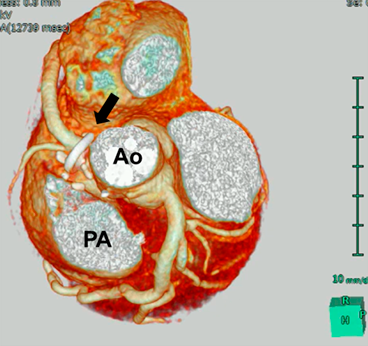
The patient’s postoperative course was uneventful. She started to take aspirin on postoperative day 1. The postoperative coronary 3D CT taken before discharge showed neither stenosis nor kinking of the reconstructed RCA (Fig. 4), and the patient was discharged on postoperative day 13. She has been asymptomatic for more than 2 years since the operation.
Anomalous aortic origin of the coronary artery (AAOCA) was first described by White and Edwards in 1948.3) The prevalence of AAORCA is reported to be 0.107% to 0.2%.4, 5) The pathomechanism of high-risk anatomic features during physical exercise includes a) kinking of the anomalous vessel with an acute-angled take-off, b) lateral compression caused by the aorta onto the intramural segment, c) intermittent closure of a slit-like orifice, and d) compression onto the interarterial portion by the aorta and the pulmonary artery.6) In our patient, c) and d) were the main causes of ischemia.
The 2018 ACHD Guideline2) states that, for anomalous aortic origin of the left coronary artery from the right sinus, surgery is reasonable even in the absence of symptoms or ischemia (class IIa). For AAORCA, on the other hand, surgery is recommended only in the presence of symptoms or diagnostic evidence consistent with coronary ischemia attributable to the anomalous coronary artery (class I). Otherwise, surgery is reasonable in the setting of ventricular arrhythmias (class IIa). In our patient, we were initially unable to detect ischemia using myocardial perfusion scintigraphy. But the cardiologist decided to check using electrocardiogram exercise testing, despite its risk of ventricular arrhythmia, after obtaining informed consent. This was because the patient’s chief complaint, exercise-related angina, seemed to be strongly related to this anomaly.
Several techniques may be used for surgical repair of AAORCA, including coronary artery bypass grafting (CABG), unroofing, reimplantation, and pulmonary arterial translocation.7, 8) CABG is a well-established technique that can be done without cardiopulmonary bypass. With this procedure, however, there is a concern regarding competitive flow at rest, and accordingly long-term patency. A short bypass using the great saphenous vein (e.g., aorta–great saphenous vein–RCA in this case) may have better patency. Moreover, myocardial infarction would not occur immediately, even if the bypass became non-patent.
The unroofing technique is the surgical option most widely used for intramural AAOCA.9) As discussed above, however, the probable pathomechanisms of ischemia in our patient were intermittent closure of the slit-like orifice and compression onto the interarterial portion by the aorta and the pulmonary artery. The unroofing technique should be effective for the type of a slit-like orifice, but would not be for the interarterial circumstance.
In contrast, reimplantation techniques can be applied to either intramural or interarterial AAOCA, and they seem to have good medium- to long-term results regarding symptom-free survival.10–12) Law et al. reported 16 cases of AAORCA repaired by reimplantation.10) Surgical reimplantation was successful in 15 patients (94%) without operative mortality, and all patients were symptom-free after surgery. Cubero et al. reported 13 cases of AAORCA11); all patients are asymptomatic and have returned to exercise without limitations. Bonilla-Ramirez et al. reported 16 cases of AAOCA12); one patient underwent CABG after reimplantation because of persistent postoperative ischemic changes, while 15 patients (94%) were released to unrestricted exercise activities. Also, a recent report has shown that the commissural manipulation associated with unroofing technique may leads to the future aortic insufficiency,13) which may support the choice of the reimplantation technique in the present patient.
Because reimplantation has a potential risk of stretching, kinking, distortion, or stenosis at the anastomosis site, it is difficult to use in patients with a small coronary artery; for example, pediatric patients or patients with a hypoplastic RCA. In our case, we chose reimplantation because the RCA was not hypoplastic but was interarterial with a slit-like ostium. The patient was 65 years old. Thus, we expected a good long-term result.
Pulmonary arterial translocation may be an alternative technique in selected cases with an anomalous course of the coronary artery as a part of complex coronary arterial anatomy; in such an occasion, the risk of coronary reimplantation may outweigh the anticipated benefits. In particular, surgical options may be limited in younger patients.14)
There are some knacks related to the reimplantation techniques, such as 1) mobilization of the RCA sparing the proximal branches of the RCA, 2) reimplantation of the RCA higher in the right facing sinus or at the very proximal ascending aorta, and 3) confirmation of correct positioning of the neo-ostium about the aortic valve commissures.15) We employed the reimplantation technique for the first time; still, the outcome seemed excellent based on adequate knowledge for these approaches obtained prior to surgery. In this sense, the reimplantation technique can be reproducibly applied to similar cases.
In conclusion, we report a case of reimplantation of the RCA in an elderly patient with AAORCA. The surgical technique used is to be selected according to the patient’s age, morphology of the coronary arteries, and other comorbidities. The reimplantation technique is useful and would be of a surgical option of choice for similar cases.
 ,Masayuki Sakaki,Tatsuya Oyama,Hiroki Mizoguchi,Nobuo SakagoshiKazuki Tanimoto
,Masayuki Sakaki,Tatsuya Oyama,Hiroki Mizoguchi,Nobuo SakagoshiKazuki Tanimoto