A levoatrial cardinal vein is a rare cardiovascular abnormality that may be present in malformed hearts with severe left heart obstruction and restrictive interatrial communication.1) This pulmonary-systemic venous connection was first described in 1926 and named in 1950 by Edwards and DuShane.2) Here, we report a newborn with a variant of hypoplastic left heart syndrome and a levoatrial cardinal vein draining into the innominate vein.
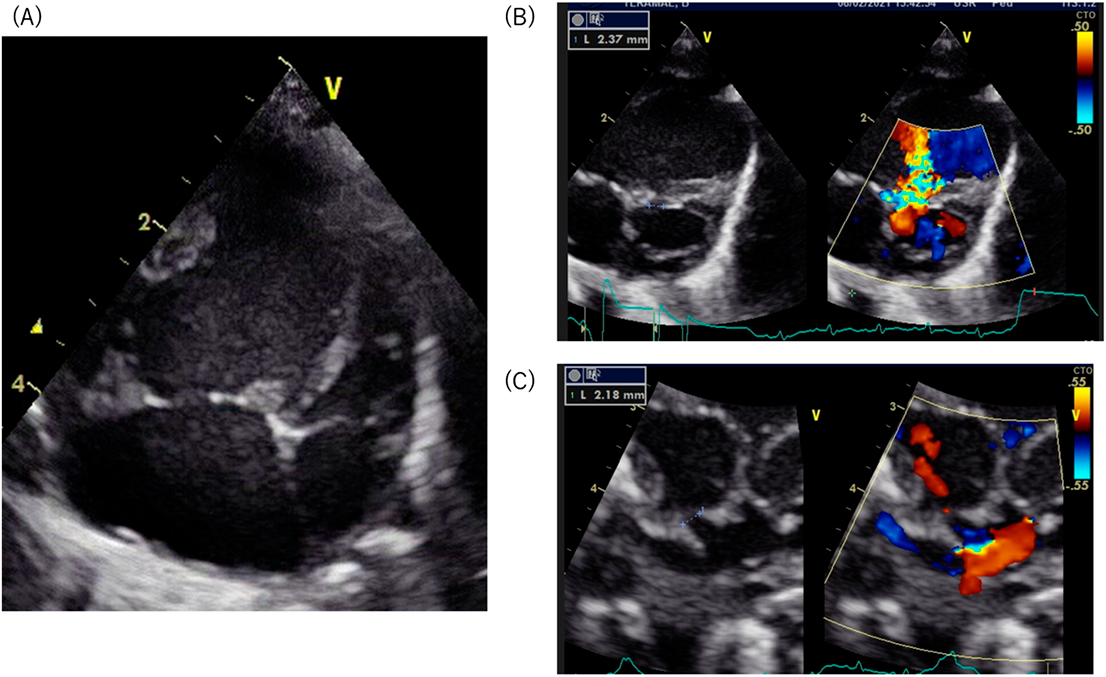
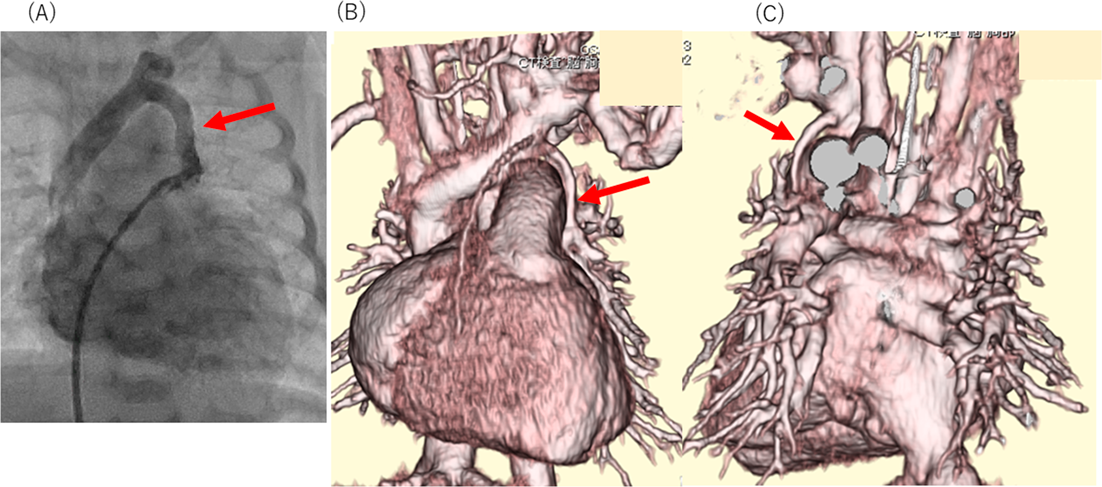
Fetal echocardiography was performed at 33 weeks of gestation at our institution, identifying a form of hypoplastic left heart syndrome with restrictive foramen ovale. The male infant was born at 38 weeks gestation via planned cesarean section, had an oxygen saturation of 89% on room air. A transthoracic echocardiography confirmed diagnosis of mitral stenosis, aortic stenosis, a small ventricular septal defect and restrictive foramen ovale (Fig. 1A–C). The four pulmonary veins were visualized, connecting to the left atrium. This patient was considered to be a candidate for the Fontan circulation in the future. Pulmonary congestion was not observed immediately after birth. We expected that pulmonary congestion should progress due to the restrictive inter-atrial communication when physiological pulmonary hypertension would decrease. This neonate underwent a balloon atrial septostomy at 1 day of age, followed by bilateral pulmonary artery banding at 2 days of age. Before performing the Norwood procedure, catheter investigation was carried out at 18 days old. This examination revealed step up of oxygen saturation at the superior vena cava; the oxygen saturation was 66%, 83%, and 93% at the inferior vena cava, the right atrium, and the superior vena cava respectively. We suspected a collateral vessel connecting the pulmonary vein to the systemic vein. Angiography of the left atrium revealed an abnormal vein draining to the innominate vein (Fig. 2A, Suppl Movie1). 3D contrast-enhanced computed tomography also showed this vein connecting the left pulmonary vein to the innominate vein (Fig. 2B, C). The abnormal vessel was identified as a levoatrial cardinal vein. The Norwood procedure was performed without ligation of this abnormal vessel. Enlargement of the atrial septal defect was performed simultaneously to avoid pulmonary congestion. The postoperative course was uneventful with no pulmonary venous obstruction.
Only a few case reports and studies have described prenatal findings of a levoatrial cardinal vein, mostly presenting in fetal hearts with severe left heart obstruction.1) Detecting this abnormality during the fetal period is considered difficult. However, when pulmonary congestion is mild, this abnormality should be considered in a postnatal echocardiographic assessment. This rare finding of a levoatrial cardinal vein represents an embryologic remnant of the fetal venous system that forms a pulmonary-systemic connection.3) Thus, the abnormal vein acts as a decompression pathway, providing an alternative egress from the left atrium for pulmonary venous blood in cardiac malformations with severe left heart obstruction. To avoid pulmonary congestion, enlargement of atrial septal defect is essential at the Norwood procedure, still we did not ligate of this vessel. Although our strategy worked well in the acute post-operative phase, this levoatrial cardinal vein is fundamentally an abnormal vessel and is not expected to work as a decompression pathway for a long time. As far as the created atrial septal defect works as a decompression pathway sufficiently, we would plan to ligate this vessel at the next surgery.
In spite of the restrictive nature of the foramen ovale in this case, the symptoms of pulmonary venous congestion was not significant. Furthermore, this patient had a small ventricular defect, that could provide another outlet for the pulmonary venous blood. Edwards and DuShane pointed out that a functionally intact atrial septum is not absolutely necessary for the formation of a levoatrial cardinal vein,2) therefore, the presence of an abnormal vein should not be ruled out, even if small interatrial or interventricular communications exist. Since accurate diagnosis is essential for determination of a treatment strategy, a multimodal imaging approach can facilitate diagnosis in the early neonatal period. The potential for a levoatrial cardinal vein must be kept in mind, even in left-sided obstructive heart disease of a variant form.
In conclusion, even in variant left heart obstruction, meticulous catheter angiography and contrast-enhanced computed tomography is mandatory to detect the presence of a levoatrial cardinal vein.
Note
Supplementary movies are provided online for this article.
Conflicts of Interest
None.
Author Contribution
All other authors have contributed to data collection and interpretation and have critically reviewed the manuscript. All authors approved the final version of the manuscript, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
引用文献References
1) Hellmund A, Berg C, Herberg U, et al: Levoatrial cardinal vein in a series of five prenatal cases with hypoplastic left heart syndrome and intact atrial septum. Ultraschall Med 2017; 2: 206–211
2) Bernstein HS, Moore P, Stanger P, et al: The levoatrial cardinal vein: Morphology and echocardiographic identification of the pulmonary-systemic connection. J Am Coll Cardiol 1995; 26: 995–1001
3) Yagel S, Kivilevitch Z, Cohen SM, et al: The fetal venous system, part I: Normal embryology, anatomy, hemodynamics, ultrasound evaluation and Doppler investigation. Ultrasound Obstet Gynecol 2010; 35: 741–750
 ,Hiroki Nagano,Yuka Hayashida,Takuya Fujisaki,Kumiyo Matsuo,Yoichiro Ishii,Hisaaki AokiMasayoshi Mori, Dai Asada
,Hiroki Nagano,Yuka Hayashida,Takuya Fujisaki,Kumiyo Matsuo,Yoichiro Ishii,Hisaaki AokiMasayoshi Mori, Dai Asada