Cardiac magnetic resonance (CMR) imaging has become essential in the management of congenital as well as acquired heart disease. High spatial resolution allows cine magnetic resonance (MR) technique to quantify chamber sizes and functions, while the velocity encoding allows phase contrast imaging to quantify blood flow at different target sites.1, 2) Significant advances in CMR studies have enhanced traditional techniques, leading to the emergence of different imaging sequences including 4-dimensional flow studies.3) Buddhe et al. reported that the median annual number of pediatric/congenital CMR cases per center in Europe and the United States was approximately 200 cases4); on the other hand, data regarding the CMR practices in Japan are still lacking among pediatric cardiologists despite the growing demand for CMR examinations even in the pediatric population. Therefore, this study aimed to clarify the current practice of CMR studies in children with either congenital or acquired heart disease in our country.
A nationwide survey was conducted by pediatric cardiologists regarding CMR practice. This study was approved by the institutional review board of the Faculty of Medicine, University of Miyazaki (approval number: C-0173). Informed consent was waived because of the nature of this study involving no personal data. Questionnaires were sent via the website to the institutions where fellows of the Japanese Society of Pediatric Cardiology and Cardiac Surgery (JSPCCS) were affiliated, asking for the number of CMR examinations according to age, disease categories, and sequence types in patients who underwent the investigation between January 1, 2022, and December 31, 2022. The disease categories were tetralogy of Fallot, post-Fontan surgery, Kawasaki disease, myocarditis/cardiomyopathy, and others. Age distributions were classified into four categories; <1 year, 1–9 years, 10–18 years, and ≥19 years. The types of image sequences included phase contrast imaging and cine MR. In addition, we asked whether sedation was required or not and also how long did it take for inage acquisition and dataset analysis. The questionnaires are shown in the supplemental Table. Responses were collected via Google Forms and compiled in a spreadsheet. To compare the distributions of age and disease categories, the Wilcoxon rank-sum test and the chi-square test were performed, respectively, using the SciPy library in Python 3. Data visualization was carried out in Excel.
There were 71 responses out of 143 institutions belonging to the JSPCCS, which accounted for a response rate of 49%. These included 12 out of 14 independent children’s hospitals belonging to the Japanese Association of Children’s Hospitals and Related Institutions. A total of 2,858 CMR examinations were performed at 51 institutions in 2022, while no CMR during the study period in the remaining 20 institutions. Only MR sequence information from 3 institutions were missing; otherwise, no missing data.
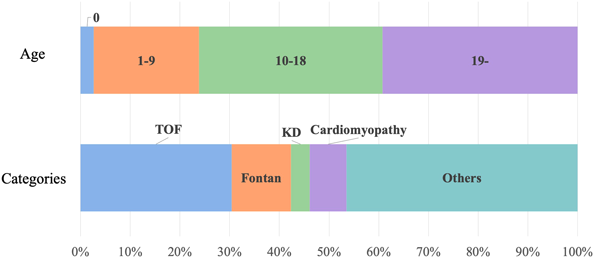
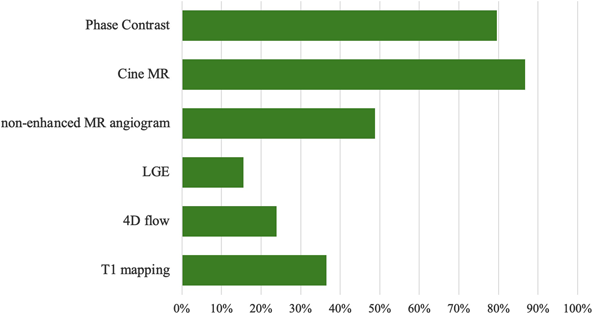
The proportions of institutions according to the number of CMR examinations are shown in Fig. 1. The median number of CMR examinations per institution was 36 per year. The number of CMR examinations was 100 or fewer in 45 institutions (89%). There were 6 institutions where more than 100 CMR studies were performed (Fig. 1). Age at CMR was <1 year in 76 patients (3%), 1–9 years in 606 (21%), 10–18 years in 1,055 (37%), and ≥19 years in 1,121 (39%) (Fig. 2). Patients aged ≥10 years accounted for 76% of all CMR examinations, so that most examinations were performed in adolescents and young adults. Regarding disease categories, the most common category was tetralogy of Fallot (TOF) (N=869, 30%), followed by postoperative Fontan (N=341, 12%), Kawasaki disease (N=108, 4%), and myocarditis and cardiomyopathy (N=211, 7%) (Fig. 2). Regarding the equipment used in each institution, 1.5-Tesla and 3-Tesla scanners were used in 34 (67%) and 17 (33%) institutions, respectively. Phase contrast imaging and cine MR were commonly used in 2,274 (80%) and 2,477 (87%) examinations, while non-enhanced magnetic resonance angiography (N=1,396, 49%), late gadolinium enhancement (LGE) (N=444, 16%), 4-dimensional flow imaging (N=684, 24%), and T1 mapping (N=1,044, 37%) were less used (Fig. 3).
Sedation was performed in 768 examinations (27%), including ventilation under endotracheal intubation in 38 examinations (1%). Intravenous sedative agents were used in 49 institutions (96%); all of these institutions reported that sedatives were given under careful observation by pediatricians. Oral sedative agents were occasionally used in 30 institutions (59%); a pediatrician attended actual investigation only in 4 institutions when oral agents were used.
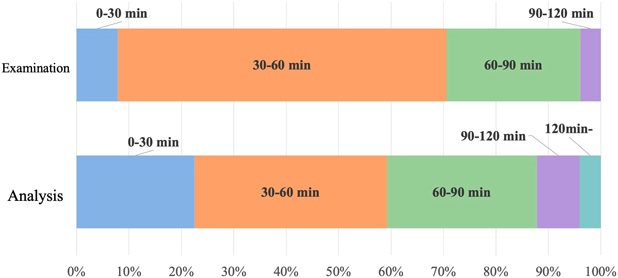
We also collected the duration of CMR examinations and that required for data analysis (Fig. 4). Thirty-two institutions (63%) reported that the CMR scanning usually took 30–60 minutes, and another 13 institutions (26%) reported as 60–90 minutes. To support image acquisition, cardiologists or pediatric cardiologists attended the examinations in 28 institutions (55%), while radiologists in 5 institutions (10%). As for data analysis, eighteen institutions (35%) reported that the process took 30–60 minutes, and another 14 institutions (28%) reported as 60–90 minutes. Medical professionals who were involved in the analysis were cardiologists/pediatric cardiologists in 35 institutions (69%), radiology technicians in 26 (51%), and radiologists in 14 (28%).
Adverse events reported were; two allergic reactions to a contrast medium, three events related to a sedation procedure that required discontinuation of the examination (e.g., respiratory depression), and 30 claustrophobic events that made the examination abandoned.
We divided institutions into two groups based on the total number of CMR examinations; ≤100 cases (N=45) and >100 cases (N=6) (Table 1). There were no significant differences in age distributions. Regarding the disease categories, tetralogy of Fallot accounted for a much higher proportion than other diseases in institutions with ≤100 CMR examinations, while the proportion of Fontan cases was greater in institutions that undertook >100 CMR examinations. A significant difference was noted in the distribution of disease categories (p<0.05). Regarding the sequences, proportions of LGE was higher in institutions with ≤100 CMR examinations, whereas the others (phase contrast, cine MR non-enhanced MR angiogram, 4D flow, T1 mapping) were more common in institutions with >100 CMR examinations. These differences showed statistical significance. Sedative procedures demonstrated no significant difference between the two groups.
Table 1 Comparison of CMR practices between institutions performing >100 vs ≤100 pediatric CMR examinations in 2022 | Institutions undertaking >100 CMR (n=6) | Institutions undertaking ≤100 CMR (n=45) | p |
|---|
| Total number of patients | 1,310 | 1,548 | |
|---|
| Age (years old) | | | n.s. |
| 0 | 39 (3.0%) | 37 (2.4%) | |
| 1–9 | 282 (21.5%) | 324 (20.9%) | |
| 10–18 | 454 (34.7%) | 601 (38.8%) | |
| 19– | 535 (40.8%) | 586 (37.9%) | |
| Disease category | | | <0.001 |
| TOF | 301 (23.0%) | 568 (36.7%) | |
| Fontan | 228 (17.4%) | 113 (7.3%) | |
| KD | 66 (5.0%) | 42 (2.7%) | |
| Cardiomyopathy | 63 (4.8%) | 148 (9.6%) | |
| Others | 652 (49.8%) | 677 (43.7%) | |
| Sequences | | | |
| Phase contrast | 1,112 (97.2%) | 1,162 (77.6%) | <0.001 |
| Cine MR | 1,129 (98.7%) | 1,348 (90.0%) | <0.001 |
| Non-enhanced MR angiogram | 959 (83.8%) | 437 (29.2%) | <0.001 |
| LGE | 167 (14.6%) | 277 (18.5%) | <0.001 |
| 4D flow | 509 (44.5%) | 175 (11.7%) | <0.001 |
| T1 mapping | 789 (69.0%) | 255 (17.0%) | <0.001 |
| Sedation | | | n.s. |
| Non-sedated | 982 (75.0%) | 1,108 (71.6%) | |
| Without endotracheal intubation | 314 (24.0%) | 416 (26.9%) | |
| With endotracheal intubation | 14 (1.1%) | 24 (1.6%) | |
| Patient age-group distribution, disease category, sequence type, and sedation method are summarized in terms of institutions performing >100 versus ≤100 CMR examinations per year. Sequence data were available for 1,144 examinations in the former group and 1,498 in the latter. CMR, cardiac magnetic resonanace; KD, Kawasaki disease; LGE, late gadolinium enhancement; MR, magnetic resonance; TOF, tetralogy of Fallot |
This study documented a questionnaire-based investigation on utilization of CMR in pediatric cardiology institutions across Japan. Our survey revealed that the median number of CMR examinations per institution was 36, substantially lower than the figure (approximately 200 examinations) reported in previous studies from the United States and Europe.4) This disparity suggests that pediatric cardiology services are less centralized in Japan, resulting in the circumstance in which accumulated experience at individual facilities would be small. Although defining the optimal model for centralized staffing is challenging, the survey of centers in North America and Europe reported 2.6–3.7 attending CMR-trained physicians per center with a median annual workload of 54–86 pediatric/congenital CMR examinations per physician. Compared to these benchmarks, both the limited number of CMR-trained personnel and the relatively low volume of clinical practice per institution are likely a major constraint on the development of pediatric CMR in Japan.
Disease Distribution and Clinical Applications
TOF was the most frequently examined condition, accounting for a quarter to one-third of all CMR examinations at each institution. This high prevalence likely reflects the routine evaluation of pulmonary regurgitation following surgical repair of TOF, that is a common indication for CMR in this patient population. The fact that TOF cases are predominant can be attributed to both its larger patient population and increasingly frequent re-interventions in this disease category. Patients following Fontan surgery represented the second most common group, underscoring the importance of hemodynamic evaluation using CMR in this population of patients with complex diseases. The remaining cases comprised various congenital heart diseases, other than TOF and Fontan cases, though specific details were not available in our survey. Given that nearly 80% of patients were older than 10 years, it is reasonable to assume that pulmonary valve diseases other than in TOF and postoperative evaluation of systemic right ventricular conditions constituted the majority of these cases. Notably, the facilities performing over 100 examinations annually demonstrated a higher proportion of Fontan patients, suggesting that more specialized centers apply CMR to a broader spectrum of complex diseases. This reflects their advanced expertise and capabilities for comprehensive patient care. In addition, imaging-sequence choices varied significantly in accordance with annual case volume. Centers performing 100 CMR studies or fewer per year relied more heavily on LGE, whereas higher-volume centers (>100 CMR studies) used hemodynamic sequences more frequently. This pattern suggests that institutions with larger CMR caseloads place greater emphasis on detailed hemodynamic assessment.
Sedation Practices
Our survey revealed striking differences in sedation practices compared to international standards. In European and the United States centers, general anesthesia involving endotracheal intubation or laryngeal mask airway is the predominant approach, utilized in 50–64% of centers.4) In contrast, our data showed that mechanical ventilation under endotracheal intubation was employed in only 1% of examinations. This finding indicates a distinctive Japanese practice favoring less invasive sedation methods for pediatric CMR, though this approach necessitates adequate remote monitoring systems to ensure patients’ safety.
Examination Duration and Supervision
The most common examination duration was 30–60 minutes, with approximately one-quarter of cases exceeding 60 minutes. This duration is consistent with previous international reports indicating a median examination time of 70–75 minutes for non-sedated patients.4) Extended examination time is attributed to the need for multiple phase contrast imaging sequences or advanced techniques such as T1 mapping in patients with complex hemodynamics. Regarding supervision, approximately 60% of facilities conducted examinations under direct observation by pediatric cardiologists or radiologists, while approximately 35% performed examinations without physician’s supervision. Given the anatomical and hemodynamic complexity of congenital heart diseases, quality control of CMR examination is critical. Examinations performed without specialist’s supervision leave a significant concern in accuracy and safety of the procedure and may require further investigation and standardization in the future.
Analysis Time and Safety Considerations
The median analysis time was substantially long, with the most common duration being 30–60 minutes. The implementation of automated analysis software, which has gained prominence in recent years, may help reduce analysis time and improve efficiency.5)
Our survey documented an extremely low complication rate. CMR examinations in sedated pediatric patients still carry inherent risks, particularly when a physician cannot be physically present near the patient. This risk is especially relevant in the Japanese context, where non-intubated sedation is more prevalent compared to in Europe and the United States; in these regions, intubated sedation accounts for more than half of all procedures. In this respect, establishing protocols for adequate remote monitoring is essential to ensure patient safety in our country.
Clinical Implications and Future Directions
Based on our findings, CMR has clearly established its position as an essential diagnostic modality in pediatric cardiology. As yet, significant variations exist in implementing practices across facilities, including differences in imaging sequences, examination protocols, and analysis procedures. Standardization of these practices between institutions would enhance the quality and the consistency of pediatric CMR service. Furthermore, centralized expertise and training programs, when developed, could help address the current disparity in examination volumes and would potentially improve overall patient care quality in pediatric cardiac imaging across Japan.
Limitations
This study has several important limitations that should be acknowledged. First, although the survey questions were developed through comprehensive discussion among the authors, no formal pretest or pilot study had been conducted to validate the questionnaire’s reliability and validity. The lack of preliminary validation may have affected the accuracy and interpretability of the collected data. Second, as a questionnaire-based survey, this study is inherently susceptible to response bias and subjective interpretation by respondents. The reliance on self-reported data may have introduced inaccuracies due to recall bias, social desirability bias, or misunderstanding of questions, potentially leading to incorrect or inconsistent responses across institutions. Third, the response rate and representativeness of participating institutions were not fully evaluated, which may limit the generalizability of our findings to all pediatric cardiology facilities in Japan. Selection bias could have occurred if institutions with more established CMR programs were more likely to participate in the survey. Fourth, the survey design did not capture temporal changes in CMR practices, as data collection represented a cross-sectional snapshot. Given the rapidly evolving nature of CMR technology and protocols, our findings may not reflect current or future practices. Finally, the lack of objective verification of reported practices represents a significant limitation. Without direct observation or audit of actual CMR procedures, discrepancies between reported and actual practices cannot be identified or quantified. Future research should address these limitations by implementing standardized survey methodologies with proper validation, incorporating objective measures of CMR practice quality, and establishing a more rigorous data collection system with enhanced quality control measures. Longitudinal studies would also provide valuable insights into the evolution of pediatric CMR practices over time.
This nationwide survey captured data from 2,858 pediatric CMR examinations across 51 centers in Japan, providing the first comprehensive overview of pediatric CMR practices in this country. Our findings revealed that Japanese pediatric cardiology institutions performed fewer CMR examinations per facility compared to international standards, with TOF being the most commonly examined condition. Notably, Japanese centers demonstrated a distinctive preference for less invasive sedation methods compared to European and American practices. The substantial variations observed in examination protocols, sedation practices, and supervision arrangements across facilities highlighted the need for standardization in pediatric CMR implementation. The overall complication rate was reassuringly low, while the frequent use of non-intubated sedation without direct physician’s supervision raised important safety matter that warrant further attention.
This study establishes a valuable baseline for pediatric CMR practices in Japan and can serve as a benchmark for individual facilities to evaluate their own performance. Furthermore, our findings provide a foundation for future surveillance studies and quality improvement initiatives in Japanese pediatric cardiac imaging. The data presented here will be instrumental in developing evidence-based guidelines for pediatric CMR practices and promoting the standardization of care across institutions nationwide.
Conflicts of Interest
The authors declare no competing interests.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contribution
All authors contributed to the study conception and design. Yoshihiko Kodama performed data collection and analysis, and wrote the first draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Note
Supplementary is provided online for this article.
引用文献References
1) Dorfman AL, Geva T, Samyn MM, et al: SCMR expert consensus statement for cardiovascular magnetic resonance of acquired and non-structural pediatric heart disease. J Cardiovasc Magn Reson 2022; 24: 44
2) Fogel MA, Anwar S, Broberg C, et al: Society for Cardiovascular Magnetic Resonance/European Society of Cardiovascular Imaging/American Society of Echocardiography/Society for Pediatric Radiology/North American Society for Cardiovascular Imaging Guidelines for the use of cardiovascular magnet. J Cardiovasc Magn Reson 2022; 24: 37
3) Itatani K, Miyazaki S, Furusawa T, et al: New imaging tools in cardiovascular medicine: Computational fluid dynamics and 4D flow MRI. Gen Thorac Cardiovasc Surg 2017; 65: 611–621
4) Buddhe S, Soriano BD, Powell AJ: Survey of centers performing cardiovascular magnetic resonance in pediatric and congenital heart disease: A report of the Society for Cardiovascular Magnetic Resonance. J Cardiovasc Magn Reson 2022; 24: 10
5) Karimi-Bidhendi S, Arafati A, Cheng AL, et al: Fully automated deep learning segmentation of pediatric cardiovascular magnetic resonance of patients with complex congenital heart diseases. J Cardiovasc Magn Reson 2020; 22: 80
 1,Kazuhiro Shiraga2,Naokazu Mizuno3,Hiroaki Urabe4,Nobuo Oyama5,Keisuke Sato6,Yoichi Iwamoto7,Kanako Kishiki8,Madoka Sawada9,Hiroshi Ono10,Akio Inage11,Kenichi Kurosaki12,Kenji Waki13,Yuichi Ishikawa14Yoshihiko Kodama
1,Kazuhiro Shiraga2,Naokazu Mizuno3,Hiroaki Urabe4,Nobuo Oyama5,Keisuke Sato6,Yoichi Iwamoto7,Kanako Kishiki8,Madoka Sawada9,Hiroshi Ono10,Akio Inage11,Kenichi Kurosaki12,Kenji Waki13,Yuichi Ishikawa14Yoshihiko Kodama