In Japan, Wolff–Parkinson–White (WPW) syndrome is detected in approximately 0.1% of all school electrocardiogram (ECG) examinations, with the latest statistics showing a rate of 0.082% across all grades.1) School ECG screening has been compulsory since 1995; children undergo ECG in their first year of primary school, junior high school, and high school. In some municipalities, additional screening is also to be performed in other grades. ECG screening is based on ECG-interpretation guidelines, and children with certain features that are extracted, including those with WPW syndrome, are instructed to visit medical institutions.2)
A certain number of schoolchildren with WPW syndrome are detected by such screening and they are eligible for follow-up. Accurate information on the risk of tachycardia should be provided for these asymptomatic patients, leading to early therapeutic intervention such as electrophysiological study (EPS). In this study, we aimed to investigate the natural history of patients with WPW syndrome detected via school ECG screening in our department, paying attention to age when attack of tachycardia first occurs and associated risk factors.
From April 2011 to December 2023, 82 patients with suspected WPW syndrome upon school ECG screening visited our department for the second screening. In these patients, the ECG was visually re-evaluated according to interpretation guidelines, and 20 patients were excluded because they did not meet diagnostic criteria such as a PR interval <0.12 s and presence of a clear delta wave. The remaining 62 patients were definitively diagnosed with WPW syndrome, and included in the study. For these patients, we confirmed their history of tachycardia symptoms according to the initial interview. No patients had been diagnosed with WPW syndrome before the school ECG examination. No patients with structural abnormalities in the heart upon echocardiography or complications from other systemic diseases were included in this study. The study was approved by the hospital’s Ethics Committee.
Tachycardia was defined as a palpitating attack with a definite onset and cessation, clearly recognized by the patient as abnormal, and confirmed via a careful interview. Patients with tachycardia attack were placed under careful observation and were indicated for medication and an EPS. Patients’ age at their first tachycardia attack and sex-related differences were also examined. Based on the most common atrioventricular accessory pathway (AVAP) location observed on the ECG, we classified patients into types A (positive delta wave in lead V1: left-sided AVAP), type B (“rS pattern” in lead V1: right-sided AVAP), and type C (“QS pattern” in lead V1: septal AVAP), and comparing the frequency of tachycardia attacks among these types.3, 4) Also investigated were differences in terms of persistent WPW syndrome (delta waves always present) and intermittent WPW syndrome (delta waves appearing intermittently). The latter was diagnosed when one or more ECGs, either at rest or for the Master two-step test, exhibited the intermittent appearance of delta waves.
The PR interval and QRS width were automatically measured and visually confirmed on ECG (ECG data-management system: EFS-8800; Fukuda Denshi, Tokyo). The delta-wave amplitude (DWA; in mm) was also measured retrospectively. It is considered useful for differentiating of fasciculo-ventricular pathways (FVPs) from the AVAP of WPW syndrome.
The DWA was defined as the maximum height of the delta waves in the first 40 ms of the most pre-excited frontal limb-lead QRS complex, according to previous reports.5, 6) The DWA was measured manually on an ECG viewer by a single, blinded author and compared between the tachycardia and the non-tachycardia groups. One additional author measured the DWA on all ECGs via the same method to assess intra-rater reliability.
Statistical Analysis
All statistical analyses were performed using EZR (Jichi Medical University Saitama Medical Center, Saitama, Japan), a software package that extends the capabilities of R and R Commander.7) Fisher’s exact test was used to compare the seizure incidence between patients with persistent WPW syndrome and those with intermittent WPW syndrome and between the sexes. Kaplan–Meier curves were constructed to compare tachycardia attacks among patients with ECG types A, B, and C, and log-rank tests were used to evaluate those differences for statistical significance. The Mann–Whitney U test was used to compare the PR interval, QRS width, and DWA between the tachycardia and the non-tachycardia groups. Spearman’s rank correlation coefficient was used to assess inter-observer variability. The normality of distributions was assessed using the Shapiro–Wilk normality test. A p-value <0.05 was considered statistically significant.
Among the 62 patients with a confirmed diagnosis of WPW syndrome, 37 (59.7%) were male. Age at diagnosis ranged from 6 to 16 years, and a median age at diagnosis was 10.5 (interquartile range: 6–13) years. The maximum follow-up period was 12 years, with a median of 4 (interquartile range: 2–6) years. In two cases, a history of tachycardia had been established at the time of the first visit. Based on the ECG features, 26 (41.9%) patients had type A, 16 (25.8%) had type B, and 20 (32.3%) had type C AVAP. Eleven patients (17.7%) had intermittent WPW syndrome.
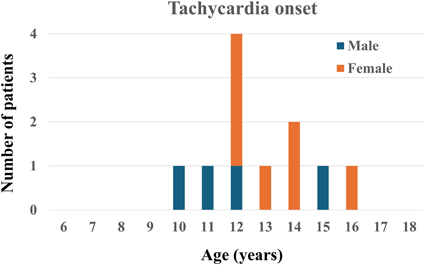
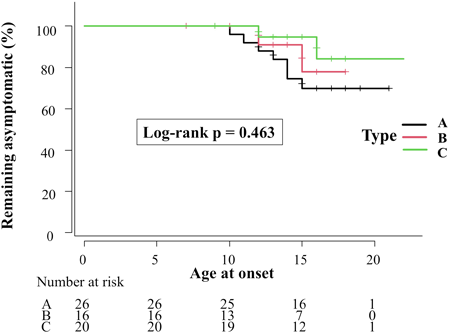
Tachycardic attack occurred in 11 (17.7%) of the 62 patients during follow-up, and the incidence of tachycardia did not differ significantly between the sexes (p=0.101; Table 1). Age at tachycardia onset ranged from 10 to 16 years old; for the largest number of patients (n=4, 36.4%), tachycardia onset occurred at the age of 12 years old (Fig. 1). Tachycardia occurred in seven patients with type A, two with type B, and two with type C AVAP (Table 1). Type A was the most prevalent; still, the three groups did not differ in terms of tachycardic attacks (p=0.463; Fig. 2). Tachycardia was not observed in the intermittent WPW syndrome group, although the difference in syndrome types did not differ statistically between patients with and without tachycardia (p=0.188; Table 1).
Table 1 Comparison based on presence or absence of tachycardia | Tachycardia (+) | Tachycardia (−) | |
|---|
| Total, n (%) | 11 (17.7) | 51 (82.3) | |
| Male, n (%) | 4 (36.3) | 33 (64.7) | p=0.101 |
| ECG type A/B/C | 7/2/2 | 19/14/18 | |
| Intermittent type | 0 | 11 | p=0.188 |
| ECG, electrocardiogram |
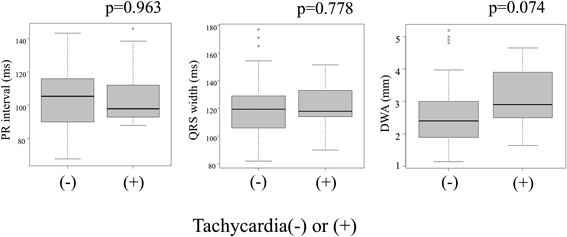
PR interval, QRS width, and DWA did not differ between the tachycardia and the non-tachycardia groups (p=0.963, p=0.778, and p=0.074, respectively; Fig. 3). The Spearman rank correlation coefficient for inter-rater reliability of the two authors for DWA measurement was 0.588 (p<0.001).
None of the 11 patients who experienced tachycardia had an ECG record of the attack.
EPS and catheter ablation was performed in six of them. Of the five patients who have not undergone EPS, one patient is awaiting it, and three patients receive antiarrhythmic drugs. The remaining one is to be followed up without medication at the patient’s request. No sudden deaths or near misses were observed in this study.
According to sources outside Japan, the prevalence of WPW syndrome is approximately 1 in 1,000 people.8–15) The proportion of male individuals in the large studies ranged from 61.0% to 68.7%, almost twice that of female individuals.8–13) Our survey revealed a similar trend, with 59.7% of patients being male.
The incidence of supraventricular tachycardia in WPW syndrome varies considerably according to study cohorts. Cain et al. in 2013 reported an incidence of 54%; obviously, they included patients with congenital heart defects, such as Ebstein’s anomaly.15) Other reports based on ECG screening, such as screening at school, revealed incidences of supraventricular tachycardia of approximately 10–20%.10–13) In a previous study on schoolchildren in Japan, the incidence of tachycardia among students with WPW syndrome was 16%.12) Similarly, in our study, the incidence of tachycardia in schoolchildren with WPW syndrome was 18%. None of the patients with intermittent WPW syndrome experienced tachycardic attacks. Although the risk of tachycardia is generally considered low in such patients, reports during the last 15 years suggested that this was not always the case.16, 17) Type A WPW appeared more common among the tachycardia group; however, the prevalence of the types did not significantly correlate with tachycardia. Therefore, clinicians should be equally cautious for all three types.
In 1990, Perry and Garson reported two peaks in the age of onset of supraventricular tachycardia in the natural history of WPW syndrome; infancy (<1 year old) and 6–8 years old. They also discovered the third and less prominent peak at approximately 13 years of age.18) This smaller peak is consistent with the peak observed in our series of patients with asymptomatic WPW syndrome detected via ECG screening, at the age of 12 years. The common finding of tachycardia around puberty suggests that several factors specific to this age group as well as physical growth may contribute to its development of tachycardia. Puberty hormones, including estrogen, thyroid hormones, growth hormones, insulin, and insulin-like growth factor 1 contribute to increased vasodilation and altered adrenergic sensitivity. Physical symptoms reflecting autonomic nervous system (ANS) dysfunction, such as vasovagal syncope and postural orthostatic tachycardia syndrome (POTS), are known to increase with the onset of puberty. Changes in the ANS during this phase of life can also affect the refractory period of atrioventricular conduction, which forms part of the reentry circuit.19–21)
We further examined the relationship between DWA and the occurrence of tachycardia, which has been reported as useful for the extraction of FVPs.22) In patients with WPW syndrome, those with certain FVPs are not at risk for tachycardia or sudden cardiac death, and thus they do not require attention. Approximately 1–5% of patients referred for EPS owing to preexcitation reportedly have FVPs.23) O’Leary et al. reported the validity of the DWA in differentiating AVAPs from FVPs. They compared the characteristics of body-surface ECGs between patients diagnosed with FVPs and those WPW syndrome with anterior septal accessory conduction pathways, reporting that a DWA >5 mm had a 96% specificity for AVAPs and a DWA <2 mm had a 96% specificity for FVPs. They suggested that an adenosine stress test would better be performed for differential diagnosis of asymptomatic patients with WPW-type ECGs and a DWA of 2–5 mm.22) The examination of the DWA in this study revealed no significant difference between patients with tachycardia and those without. Although FVPs were estimated to be prevalent in the non-tachycardia group, the DWA was not a significant predictor of tachycardia. Furthermore, although the inter-rater agreement was significant between two of the authors, the level of agreement was not satisfactory. This fact raises concerns about inter-rater variability in manual measurements.
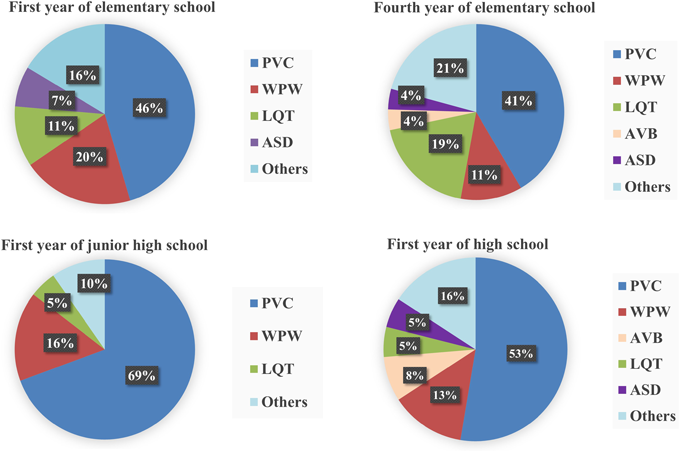
WPW syndrome is an important finding in ECG screening at school, often resulting in early diagnosis and management. For reference, we also present the proportion of diseases diagnosed in schoolchildren who underwent such a screening and visited our hospital for management from 2012 to 2020 (Fig. 4). Of the 1,754 patients who visited the department, 346 (19.7%) patients required management. Among those 346, WPW syndrome was the second most frequent diagnosis after premature ventricular contraction in key grades, comprising 20% in the first year of elementary school, 16% in the first year of junior high school, and 13% in the first year of high school.
Many of patients with WPW syndrome remain asymptomatic, and outpatient management strategies are likely to vary among healthcare facilities. We inform the patients and their parents about the pathogenesis of WPW syndrome and the probable symptoms at the first visit. Then, we instruct them to seek medical attention once symptom occurs. ECG recording during tachycardic attacks is often difficult to obtain, and decisions for treatment are usually based on patient complaints. We explain to the patients and their parents how to measure their pulse. We indicate them to monitor patient’s heart rate during a tachycardic episode so that the attack can be confirmed objectively. We believe that information about age when patients are most likely to experience an attack should also be provided to ensure a prompt response in case symptoms occur.
This study has some limitations that should be considered. First, this was a single-center study with a small sample size. Second, we relied solely on symptom-based interviews, which might not have been sufficient to detect tachycardia in younger patients who could not describe their symptoms. Furthermore, other causes of tachycardic attacks, such as ANS disorders, including POTS, cannot be completely ruled out. In recent years, many reports have been published on the usefulness of wearable terminal, which are becoming increasingly popular, for the observation of heart-rate waveforms. We expect that they will be incorporated into diagnosis of tachycardic attacks.24)
In this study, the most common age at tachycardia onset was approximately 12 years old. Predicting the risk of tachycardic attacks was difficult from ECG waveforms alone. Although most patients with WPW syndrome detected through school-based examinations are asymptomatic for the time being, regular checkup is recommended, especially around the age when tachycardia tends to occur.
謝辞Acknowledgments
The authors would like to thank all the workers in our pediatric department and those involved in school screening for their support. We thank Honyaku Center Inc. for English language editing.
Conflicts of Interest
The authors declare no competing interests.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Fukui Cardiovascular Center. Approval No. 2024-012.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article.
Author Contribution
Conceptualization: Koichi Nishida
Data curation: Koichi Nishida, Shintaro Okazaki, and Satoshi Tamura
Formal analysis: Koichi Nishida
Investigation: Koichi Nishida, Shintaro Okazaki, and Satoshi Tamura
Supervision: Shintaro Okazaki and Satoshi Tamura
Visualization: Koichi Nishida
Writing — original draft: Koichi Nishida
Writing — review & editing: Koichi Nishida, Shintaro Okazaki, and Satoshi Tamura
引用文献References
1) Tokyo Health Service Association: Tokyo Preventive Medicine Association Activity Report No. 52. 2024. Available from https://www.yobouigaku-tokyo.or.jp/nenpo/pdf/2024/04.pdf
2) Sumitomo N, Baba R, Doi S, et al: Japanese Circulation Society and the Japanese Society of Pediatric Cardiology and Cardiac Surgery of Joint Working: Guidelines for heart disease screening in schools (JCS 2016/JSPCCS 2016)—Digest Version—. Circ J 2018; 82: 2385–2444
3) Rosenbaum FF, Hecht HH, Wilson FN, et al: The potential variations of the thorax and the esophagus in anomalous atrioventricular excitation (Wolff-Parkinson-White syndrome). Am Heart J 1945; 29: 281–326
4) Ueda H, Nameki C, Saruta H, et al: Further studies on the W.P.W. syndrome (pre-excitation syndrome) with special reference to the intracardiac and esophageal lead. Jpn Circ J 1957; 21: 361–375
5) Gallagher JJ, Smith WM, Kasell JH, et al: Role of Mahaim fibers in cardiac arrhythmias in man. Circulation 1981; 64: 176–189
6) Fitzpatrick AP, Gonzales RP, Lesh MD, et al: New algorithm for the localization of accessory atrioventricular connections using a baseline electrocardiogram. J Am Coll Cardiol 1994; 23: 107–116
7) Kanda Y: Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48: 452–458
8) Hiss RG, Lamb LE: Electrocardiographic findings in 122,043 individuals. Circulation 1962; 25: 947–961
9) Munger TM, Packer DL, Hammill SC, et al: A population study of the natural history of Wolff-Parkinson-White syndrome in Olmsted County, Minnesota, 1953–1989. Circulation 1993; 87: 866–873
10) Goudevenos JA, Katsouras CS, Graekas G, et al: Ventricular pre-excitation in the general population: A study on the mode of presentation and clinical course. Heart 2000; 83: 29–34
11) Santinelli V, Radinovic A, Manguso F, et al: Asymptomatic ventricular preexcitation: A long-term prospective follow-up study of 293 adult patients. Circ Arrhythm Electrophysiol 2009; 2: 102–107
12) Sano S, Komori S, Amano T, et al: Prevalence of ventricular preexcitation in Japanese schoolchildren. Heart 1998; 79: 374–378
13) Fitzsimmons PJ, McWhirter PD, Peterson DW, et al: The natural history of Wolff-Parkinson-White syndrome in 228 military aviators: A long-term follow-up of 22 years. Am Heart J 2001; 142: 530–536
14) Janson CM, Millenson ME, Okunowo O, et al: Incidence of life-threatening events in children with Wolff-Parkinson-White syndrome: Analysis of a large claims database. Heart Rhythm 2022; 19: 642–647
15) Cain N, Irving C, Webber S, et al: Natural history of Wolff-Parkinson-White syndrome diagnosed in childhood. Am J Cardiol 2013; 112: 961–965
16) Kiger ME, McCanta AC, Tong S, et al: Intermittent versus persistent Wolff-Parkinson-White syndrome in children: Electrophysiologic properties and clinical outcomes. Pacing Clin Electrophysiol 2016; 39: 14–20
17) Cohen MI, Triedman JK, Cannon BC, et al: Pediatric and Congenital Electrophysiology Society (PACES); Heart Rhythm Society (HRS); American College of Cardiology Foundation (ACCF); American Heart Association (AHA); American Academy of Pediatrics (AAP); Canadian Heart Rhythm Society (CHRS): PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: Developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS). Heart Rhythm 2012; 9: 1006–1024
18) Perry JC, Garson A Jr.: Supraventricular tachycardia due to Wolff-Parkinson-White syndrome in children: Early disappearance and late recurrence. J Am Coll Cardiol 1990; 16: 1215–1220
19) Coupal KE, Heeney ND, Hockin BCD, et al: Pubertal hormonal changes and the autonomic nervous system: Potential role in pediatric orthostatic intolerance. Front Neurosci 2019; 13: 1197
20) Roberts JM, Insel PA, Goldfien A: Regulation of myometrial adrenoreceptors and adrenergic response by sex steroids. Mol Pharmacol 1981; 20: 52–58
21) Shen MJ, Zipes DP: Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ Res 2014; 114: 1004–1021
22) O’Leary ET, Dewitt ES, Mah DY, et al: Differentiation of fasciculoventricular fibers from anteroseptal accessory pathways using the surface electrocardiogram. Heart Rhythm 2019; 16: 1072–1079
23) Ratnasamy C, Khan D, Wolff GS, et al: Clinical and electrophysiological characteristics of fasciculoventricular fibers in children. Int J Cardiol 2008; 123: 257–262
24) Hughes A, Shandhi MMH, Master H, et al: Wearable devices in cardiovascular medicine. Circ Res 2023; 132: 652–670
 1,Shintaro Okazaki1,Satoshi Tamura2Koichi Nishida
1,Shintaro Okazaki1,Satoshi Tamura2Koichi Nishida