Aortic valve neocuspidization (AVNeo) has garnered considerable acceptance within the adult population.1–3) Numerous reports have indicated the feasibility of implementing AVNeo in pediatric patients; however, the inherent challenges of this technique remain inadequately elucidated.4–6) Herein, we present a case in which AVNeo was attempted but ultimately necessitated conversion to mechanical valve replacement accompanied by annular enlargement.
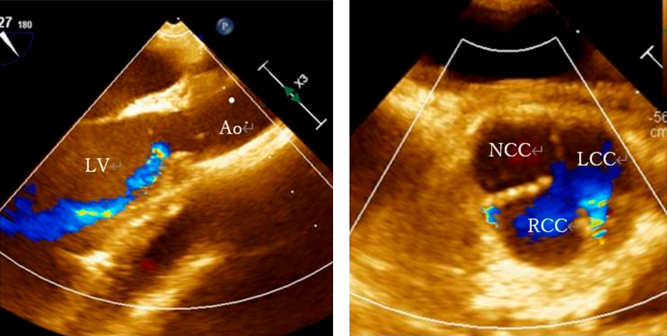
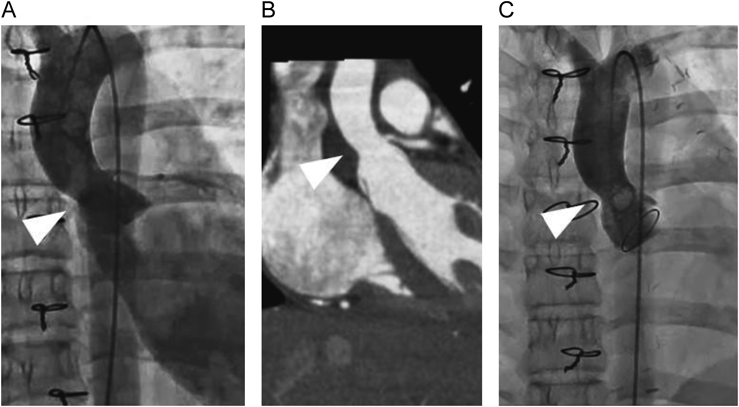
A 12-year-old girl with an anomalous origin of the left coronary artery from the right coronary cusp, characterized by intramural course of the coronary artery, underwent unroofing of the left main trunk. During the surgical procedure, aortic regurgitation (AR) emerged, prompting us to attempt commissural suspension and plasty to the right coronary cusp. Despite the aortic valve intervention included within a total cardiac arrest duration of 174 minutes, a trivial-mild degree of AR persisted. Subsequently, AR through the central and commissural regions between the left and the right coronary cusps progressively deteriorated (Fig. 1). The left ventricular end-diastolic diameter increased from 42 mm to 45 mm over a period of six months. Cardiac catheterization performed three months postoperatively revealed left ventricular end-diastolic pressure of 16 mmHg, AR being categorized as Sellers IV. Despite the absence of a discernible pressure gradient, morphological constriction was noted at the sino-tubular junction (Fig. 2A). Additionally, contrast-enhanced computed tomography confirmed the narrowing of the sino-tubular junction (Fig. 2B). Given the patient’s age and activity level, we considered AVNeo as a viable alternative to mechanical valve replacement.
Following dissection around the heart, the pericardium was harvested and subjected to glutaraldehyde treatment for seven minutes. After induction of cardioplegic arrest, a transverse aortotomy was performed in the proximal ascending aorta, approximately 1.5 cm distal to the right coronary ostium. All three leaflets exhibited thickening, particularly the left coronary cusp, necessitating complete resection. The dimension of the non-coronary cusp was measured 17 mm, and 15 mm each for the right and the left coronary cusps. Three new aortic valve leaflets were meticulously fashioned from the glutaraldehyde-treated autologous pericardium using a commercially available template. Subsequently, these were sutured to the remnant hinges of the resected leaflets and the aortic wall (Fig. 3). The aortotomy was reinforced with a patch of the glutaraldehyde-treated autologous pericardium. During the weaning process from cardiopulmonary bypass, ventricular fibrillation occurred frequently. Direct pressure measurements indicated that left atrial pressure exceeded 30 mmHg, while transesophageal echocardiography revealed diminished left ventricular contractility. The peak flow velocity across the aortic valve was measured as 4.1 m/s. Consequently, cardiac arrest was induced again; the previous aortotomy was extended into the non-coronary sinus, the reconstructed leaflets were all excised, and a 17 mm St. Jude Medical Regent valve (St. Jude Medical, St. Paul, MN) was positioned in the supra-annular location following aortic annular enlargement by the Nicks procedure. Subsequent to this revision, weaning from cardiopulmonary bypass was successfully achieved, and an estimated pressure gradient across the aortic valve became less than 20 mmHg. (The first aortic cross-clamp time was 186 minutes, and the second 143 minutes.) After a prolonged 10-day intensive care unit stay due to persistent pleural effusion, the patient was discharged home on the postoperative day 25.
At the four-month postoperative assessment, cardiac catheterization revealed morphological constriction of the sino-tubular junction (Fig. 2C). On the other hand, trans-thoracic echocardiography did not indicate aortic stenosis; a peak velocity (Vmax) of 0.8 m/s and a mean pressure gradient (PG) of 2 mmHg.
Recent literature has documented an increasing number of pediatric cases of AVNeo, some demonstrating superior short-term outcomes compared to mechanical valve replacement. The advantages of AVNeo in the pediatric demographics include the elimination of anticoagulant requirements, the absence of an immune response to autologous pericardium-derived valve leaflets, and the prevention of prosthesis-patient mismatch associated with the implantation of prosthetic valves within a diminutive valve annulus.3–5) In this case, the implantation of a bioprosthetic valve was deemed unfeasible due to the limited size of the aortic annulus. Additionally, lifelong anticoagulation following mechanical valve implantation must be avoided due to its teratogenic potential. Furthermore, the Ross procedure was precluded by the patient’s anomalous coronary arterial anatomy. Thus, AVNeo emerged as the most favorable surgical option.
The diameter of the aortic annulus was measured as 19 mm (Z=0.24), indicating that the annular size itself did not contraindicate AVNeo. However, limited motion of the reconstructed leaflets would have been anticipated for two reasons. Firstly, anatomy of the aortic root were significantly unusual. The core concept of AVNeo involves reconstructing aortic valve cusps using oversized pericardial leaflets to achieve optimal coaptation. Given her morphologically constricted sino-tubular junction, it was hypothesized that redundant leaflet tissues might have encountered restrictions in movement at this anatomical juncture. Additionally, it was conceivable that the thickened new aortic valve leaflets could have covered the coronary arterial orifices causing cardiac ischemia and ventricular fibrillation following aortic declamping. In the adult population, in contrast, both stenosis and regurgitation across the aortic valve typically result in dilation of the aortic root, including the sino-tubular junction, wherein redundant reconstructed leaflets would function optimally. The etiology of stenosis in our patient remains unknown; we speculate that a prior surgical intervention could have promoted this lesion. While we were aware of the aortic constriction preoperatively, we opted against intervention on the lesion, as both cardiac catheterization and echocardiography indicated no significant pressure gradient. In this patient, the initial aortic clamp time was 186 minutes, which was excessively prolonged to repeat aortic cross-clamp for further aggressive augmentation. Therefore, we opted for aortic valve replacement as it presented a more reliable and expedient solution rather than sticking to AVNeo. AVNeo concomitantly with alleviation of supra-aortic stenosis from the beginning might have yielded better outcomes. This would be particularly the case in patients undergoing AVNeo at reoperations.
Secondly, it is debatable whether use of the autologous pericardium is appropriate for AVNeo at reoperation. Watanabe et al. have documented leaflet degeneration following AVNeo in pediatric patients, with one patient developing intraoperative moderate aortic stenosis.6) This particular patient had a surgical history prior to AVNeo and presented with a small aortic annulus (95% of the normal size). The authors postulated that inadequate pericardial flexibility led to aortic stenosis, which manifested during the postoperative period. Although the harvested autologous pericardium appeared pliable, it could have been less ideal for long-lasting AVNeo leaflets. Use of alternative materials, such as a bovine pericardium, might have enhanced mobility of reconstructed leaflets.
Furthermore, the etiology of aortic regurgitation in our case is likely iatrogenic, stemming from alterations in the geometry of the right coronary cusp during the previous surgical intervention. Direct inspection during AVNeo revealed degeneration of all three leaflets around the central edges and a central jet had been noted on preoperative echocardiography. Still, the primary cause of regurgitation was identified as prolapse of the right coronary cusp. Consequently, single-leaflet reconstruction would have been a plausible alternative.7)
AVNeo was performed in an adolescent, culminating in intraoperative conversion to mechanical valve replacement. Hemodynamically inconsequential but morphologically significant supra-aortic stenosis and creation of new aortic leaflets derived from the thickened and inflexible autologous pericardium resulted in severe aortic valve obstruction intraoperatively. When AVNeo is carried out as a reoperation, supra-aortic stenosis would better be addressed and use of degenerative/thickened autologous pericardium should be avoided in order to enhance the outcomes of AVNeo. Additionally, single-leaflet reconstruction may represent a viable alternative, particularly in such instances.
Conflicts of Interest
The authors have no competing interests to declare.
Ethical Declarations
Ethics approval and consent to participate are not applicable. Her parent permitted the utilization of her personal data for the development of medical science (11/07/2023).
Author Contribution
YF wrote the manuscript (original draft) and contributed to the creation of the figures and table. TH and TS supervised and authorized this study. TN, AH, HN and YI performed the surgery and/or perioperative patient management. All authors read and approved the manuscript.
Availability of Data and Materials
No additional data.
引用文献References
1) Ozaki S, Kawase I, Yamashita H, et al: Aortic valve reconstruction using autologous pericardium for patients aged less than 60 years. J Thorac Cardiovasc Surg 2014; 148: 934–938
2) Iida Y, Fujii S, Akiyama S, et al: Early and mid-term results of isolated aortic valve neocuspidization in patients with aortic stenosis. Gen Thorac Cardiovasc Surg 2018; 66: 648–652
3) Amabile A, Krane M, Dufendach K, et al: Standardized aortic valve neocuspidization for treatment of aortic valve diseases. Ann Thorac Surg 2022; 114: 1108–1117
4) Baird CW, Cooney B, Chávez M, et al: Congenital aortic and truncal valve reconstruction using the Ozaki technique: Short-term clinical results. J Thorac Cardiovasc Surg 2021; 161: 1567–1577
5) Marathe SP, Chávez M, Sleeper LA, et al: Modified Ozaki procedure including annular enlargement for small aortic annuli in young patients. Ann Thorac Surg 2020; 110: 1364–1371
6) Watanabe F, Go K, Kojima T: Valvular changes after aortic valve neo-cuspidization in children: A case series. Pediatr Int 2021; 63: 1289–1296
7) Marathe SP, Chávez M, Sleeper LA, et al: Single-leaflet aortic valve reconstruction utilizing the Ozaki technique in patients with congenital aortic valve disease. Semin Thorac Cardiovasc Surg 2022; 34: 1262–1272
 1,Taisuke Nabeshima2,Akinori Hirano1,Haruhiro Nagase1,Yukino Iijima1,Takaaki Suzuki1Yuji Fuchigami1, Takaya Hoashi
1,Taisuke Nabeshima2,Akinori Hirano1,Haruhiro Nagase1,Yukino Iijima1,Takaaki Suzuki1Yuji Fuchigami1, Takaya Hoashi