11.4. CQ 3: Are 3D/4D Images Effective for Screening/Diagnosing FHD?
発行日:2023年12月1日Published: December 1, 2023
© 2023 特定非営利活動法人日本小児循環器学会© 2023 Japanese Society of Pediatric Cardiology and Cardiac Surgery
Fetal echocardiography is typically performed using 2D imaging. Recent advancements in ultrasound equipment have made it easier to obtain 3D and 4D images. During examinations of pregnant women, the face and the body of the fetus are frequently observed using 3D imaging. During fetal echocardiography, STIC (spatiotemporal image correlation) developed for the fetal heart can construct a 3D/4D image based on the fetal heart rate by simply scanning the fetal heart for approximately 10 seconds. This allows observation of the 3D structure of the heart. In the screening involving STIC, it is common to display the 4CV, the 3VV, and the 3VTV horizontal cross-sections of the fetus using the tomographic ultrasound imaging (TUI) function. These findings are usually considered comparable to those by the 2D examination procedures.
Use of 3D/4D images for screening/diagnosing FHD has been attempted, but yet to be clarified in their real usefulness. This is the current point under the CQ “Are 3D/ 4D images effective for screening/diagnosing FHD?”
The effect of 3D/4D images on the detection rate and the diagnosis rate was determined in screening/diagnosing FHD. To clarify the points of discussion, the outcomes were set at a couple of aspects; that is, comparison of the detection rate of cardiac structures between on 2D images and on 3D/4D images, and the impact on the detection rate of cardiac structural abnormalities when 3D/4D images are applied.
At the primary extraction, included were 233 articles focused on screening/diagnosing FHD using 3D/4D images. Of those, 60 articles were included at the stage of the secondary extraction. Five reports fulfilled the final criteria. Of those five, three focused on the comparison of the detection rate of cardiac structures between on 2D images and on 3D/4D images.1–3) The remaining two focused on the increase in the detection rate of cardiac structural abnormalities with 3D/4D images.1, 4)
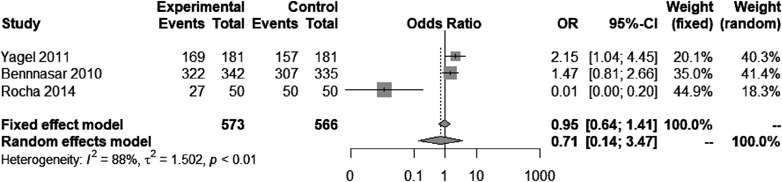
Three studies were scrutinized in which the detection rate on 3D/4D modality was compared to that with 2D images only. One study3) included healthy participants, another2) included patients with heart diseases, and the third1) included both. In these three studies, TUI was used for 3D/4D images. During the meta-analysis, the heterogeneity of the test results was considered, and the overall evidence was described using random effects. The CI of the OR for the detection rate of heart structures overlies 1.0. There was no significant difference between the detection rate on 3D/4D images and that on 2D images only (OR, 0.71; 95% CI, 0.14–3.47; p=0.66).
Two out of these three studies reported the superiority of the 3D/4D technology. The study by Bennasar et al.1) reported that the sensitivity rates of 2D images and 3D/4D images were 98.3% and 94.9%, respectively, and the specificity rates 89.8% and 88.1%, respectively; namely, no significant differences. Among the nine false-negative results obtained using 3D/4D images, ventricular septal defect was the malformation in 8, and severe heart disease (interruption of the aortic arch) in the remaining one. In the study by Yagel et al.,2) the sensitivity rate was 87.5% and the specificity rate was 100% for 2D images only. The sensitivity rate increased to 93.7% with the addition of 3D/4D images, indicating that combining 2D and 3D/4D images were useful.
It takes approximately 10 seconds for scanning the entire heart in the 4CV on 3D/4D images. Because of the duration of time, the outflow tract may be difficult to see due to fetal movements, the fetal position, and the position of the spine.3) This makes the detection rate of cardiac structures on 3D/4D images lower than that of 2D images. Two studies1, 2) judged that large biases lay in the examination methods and the patient selection. In either of these studies, color Doppler imaging and bidirectional power Doppler imaging were used without setting exclusion criteria for 3D/4D data when the outflow tract was not well illustrated. Some patients could have been excluded from the beginning whose cardiac structures were difficult to visualize due to fetal movement or its position.
With these factors into account, a favorable impact of 3D/4D images onto the detection rate during the screening stage remains unclear, at least at present, comparing to the conventional 2D technique alone.
Two reports1, 4) were evaluated to determine whether the detection rate of structural abnormalities is higher using 3D/4D images. TUI was the method to express 3D/4D images in either of these studies. Heterogeneity was insignificant, but the overall evidence was described as random effects. The CI of the OR expanded over 1.0. It cannot be concluded that 3D/4D images are more capable of depicting intracardiac abnormal structures than the conventional images do (OR, 1.16; 95% CI, 0.26–5.44; p=0.85).
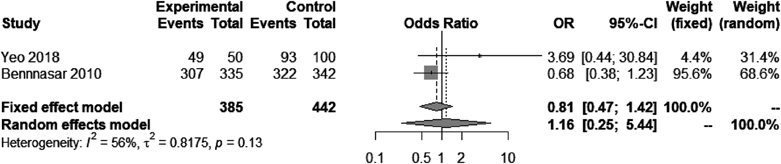
These studies by Yeo et al.4) and Bennasar et al.1) indicated conflicting results regarding the detection rate of structural abnormalities. Their results seemed greatly affected by the number of patients with heart diseases (mainly ventricular septal defect). Yeo et al.4) included only two patients (4%) with ventricular septal defect, and the heart problem was securely detected in these patients. In contrast, Bennasar et al.1) included 38 patients (22%) with ventricular septal defect. The heart lesion was not noted in eight out of these patients. Only one patient had an interrupted aortic arch among their cohort of patients. Further investigation is necessary to clarify the circumstances with such significant heart diseases that should cause clinical problems immediately after birth.
Additionally, use of 4D surface rendering images, xPlane, or 4D-B-flow may enable to evaluate and diagnose abnormalities of the fetal semilunar valve and mitral valve. Diagnostic applications of these methods have also been reported in vascular abnormalities such as transposition of the great arteries and tetralogy of Fallot.5–7) Furthermore, a couple of studies8, 9) evaluated whether 3D/4D imaging was reproducible and prompt enough. Reproducibility appeared promising with experienced examiners. As for time consumption, the reports stated that the analysis could be established within a routine duration of time regardless of the experience level of the examiner. Importantly, there were no adverse events associated with 3D/4D imaging.
At present, it is not quite evident that 3D/4D imaging is effective for detecting cardiac structural abnormalities at the screening stage. Favorable aspects are no obvious adverse events foreseen, reproducibility promising, and the procedure not time-consuming. It is expected that structural abnormalities will be captured with a higher sensitivity in the future by using 3D/4D imaging with improved performance of ultrasound scan, with advanced skills of the examiners, and with sophisticated analysis software.
Little evidence was available for supporting useful application of 3D/4D images in screening/diagnosing FHD. The ability to depict the normal structures of 3D/4D imaging was not superior to that of 2D images. Not for the detection rate of structural abnormalities of the fetal heart, either. Therefore, the evidence level is D (very weak).
It is good to know that there are no reports of adverse events associated with 3D/4D imaging. Reproducibility of the findings seems favorable, so does time consumption of the examination. It is hopeful that combining 3D/4D imaging with 2D imaging would improve the detection rate of heart disease, admitting that the examiner’s experience/skill and the fetal position/movement should affect the detection rates for fetal cardiac disease and cardiac structural abnormalities in clinical settings where 3D/4D equipment is available. Overall, adding 3D/4D imaging to 2D modality is not unreasonable.
Fetal echography is typically performed using 2D imaging. Recently, use of ultrasound equipment capable of depicting 3D and 4D images has become widespread at facilities of maternal-fetal medicine. The 3D images are mainly used to observe the fetal face and body. In addition, 3D/4D images of the fetal heart can be easily obtained using STIC, which has been developed for the fetal heart. This device can be used for the screening and diagnosis of FHD.
The CQ “Are 3D/4D images effective for screening/diagnosing FHD?” was set to organize the findings and determine the level of recommendations.
Currently, the ability to detect FHD on 3D/4D images is not comparable to that on 2D images. Solitary use of 3D/4D images is not recommended for screening/diagnosing FHD. Nonetheless, a downside of using 3D/4D images for this purpose is simply to increase the examination time by approximately 10 minutes. Performing both 3D/4D and 2D imaging can raise the detection rate of FHD. How accurately the examination describes the fetal circumstance depends on the movement and the position of the fetus as well as the skill of the examiner. With this in mind, it is reasonably recommended that 3D/4D imaging is to be applied together with 2D imaging when considered appropriate.
1) Bennasar M, Martínez JM, Gómez O, et al: Accuracy of four-dimensional spatiotemporal image correlation echocardiography in the prenatal diagnosis of congenital heart defects. Ultrasound Obstet Gynecol 2010; 36: 458–464
2) Yagel S, Cohen SM, Rosenak D, et al: Added value of three-/four-dimensional ultrasound in offline analysis and diagnosis of congenital heart disease. Ultrasound Obstet Gynecol 2011; 37: 432–437
3) Rocha LA, Rolo LC, Barros FS, et al: Assessment of quality of fetal heart views by 3d/4d ultrasonography using spatiotemporal image correlation in the second and third trimesters of pregnancy. Echocardiograph 2014; 32: 1015–1022
4) Yeo L, Luewan S, Romero R: Fetal Intelligent Navigation Echocardiography (FINE) detects 98% of congenital heart disease. J Ultrasound Med 2018; 37: 2577–2593
5) Hu G, Zhang Y, Fan M, et al: Evaluation of fetal cardiac valve anomalies by four-dimensional echocardiography with spatiotem- poral image correlation. Echocardiography 2016; 33: 1726–1734
6) Xiong Y, Liu T, Gan HJ, et al: Detection of the fetal conotruncal anomalies using real-time three-dimensional echocardiography with live xPlane imaging of the fetal ductal arch view. Prenat Diagn 2013; 33: 462–466
7) Zhang D, Zhang Y, Ren W, et al: Prenatal diagnosis of fetal interrupted aortic arch type a by two-dimensional echocardiography and four-dimensional echocardiography with b-flow imaging and spatiotemporal image correlation. Echocardiography 2015; 33: 90–98
8) Wang N, Xie HN, Peng R, et al: Accuracy, agreement, and reliability of fetal cardiac measurements using 4-dimensional spatiotemporal image correlation. J Ultrasound Med 2012; 31: 1719–1726
9) Novaes JY, Zamith MM, Araujo Júnior E, et al: Screening of congenital heart diseases by three-dimensional ultrasound using spatiotemporal image correlation: Influence of professional experience. Echocardiography 2016; 33: 99–104
This page was created on 2022-12-26T16:45:22.593+09:00
This page was last modified on 2023-11-27T10:50:40.000+09:00
このサイトは(株)国際文献社によって運用されています。
